

Randomized trial of stopping or continuing ART among postpartum women with pre-ART CD4 ≥ 400 cells/mm3
- PMID: 28489856
- PMCID: PMC5425014
- DOI: 10.1371/journal.pone.0176009
Randomized trial of stopping or continuing ART among postpartum women with pre-ART CD4 ≥ 400 cells/mm3
Abstract
Background: Health benefits of postpartum antiretroviral therapy (ART) for human immunodeficiency virus (HIV) positive women with high CD4+ T-counts have not been assessed in randomized trials.
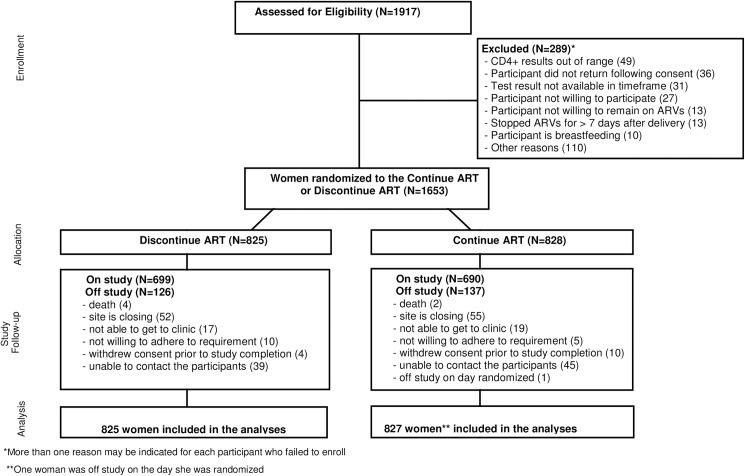
Methods: Asymptomatic, HIV-positive, non-breastfeeding women with pre-ART CD4+ T-cell counts ≥ 400 cells/mm3 started on ART during pregnancy were randomized up to 42 days after delivery to continue or discontinue ART. Lopinavir/ritonavir plus tenofovir/emtricitabine was the preferred ART regimen. The sample size was selected to provide 88% power to detect a 50% reduction from an annualized primary event rate of 2.07%. A post-hoc analysis evaluated HIV/AIDS-related and World Health Organization (WHO) Stage 2 and 3 events. All analyses were intent to treat.
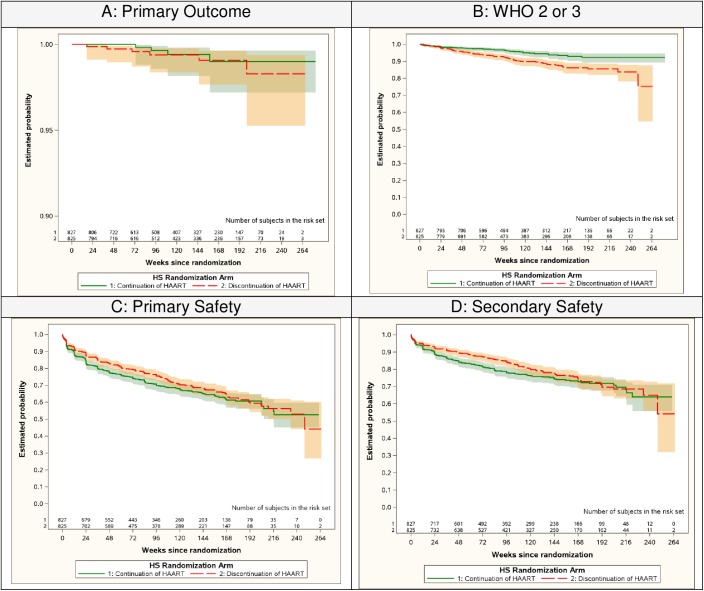
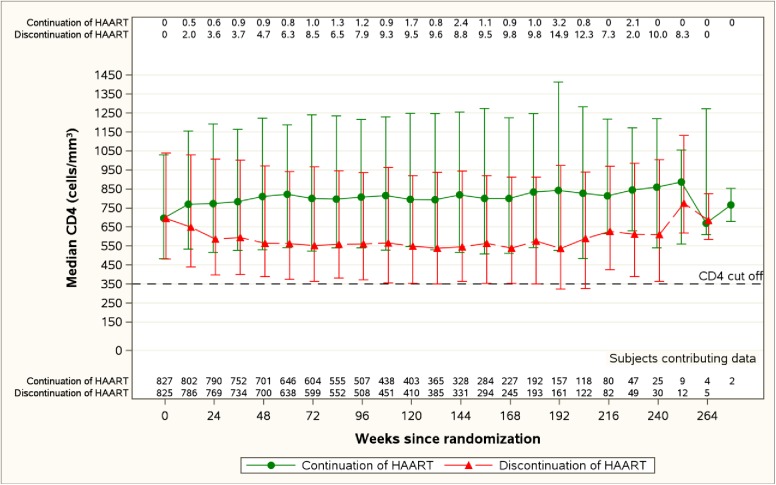
Results: 1652 women from 52 sites in Argentina, Botswana, Brazil, China, Haiti, Peru, Thailand and the US were enrolled (1/2010-11/2014). Median age was 28 years and major racial categories were Black African (28%), Asian (25%) White (15%). Median entry CD4 count was 696 cells/mm3 (IQR 575-869), median ART exposure prior to delivery was 19 weeks (IQR 13-24) and 94% had entry HIV-1 RNA < 1000 copies/ml. After a median follow-up of 2.3 years, the primary composite endpoint rate was significantly lower than expected, and not significantly different between arms (continue arm 0.21 /100 person years(py); discontinue 0.31/100 py, Hazard ratio (HR) 0.68, 95% CI: 0.19, 2.40). WHO Stage 2 and 3 events were significantly reduced with continued ART (2.08/100 py vs. 4.36/100 py in the discontinue arm; HR 0.48, 95%CI: 0.33, 0.70). Toxicity rates did not differ significantly between arms. Among women randomized to continue ART, 189/827 (23%) had virologic failure; of the 155 with resistance testing, 103 (66%) failed without resistance to their current regimen, suggesting non-adherence.
Conclusions: Overall, serious clinical events were rare among young HIV-positive post-partum women with high CD4 cell counts. Continued ART was safe and was associated with a halving of the rate of WHO 2/3 conditions. Virologic failure rates were high, underscoring the urgent need to improve adherence in this population.
Trial registration: ClinicalTrials.gov NCT00955968.
Conflict of interest statement
Figures
References
-
- Govender T, Coovadia H. Eliminating mother to child transmission of HIV-1 and keeping mothers alive: recent progress. J Infect 2014; 68 Suppl 1: S57–62. - PubMed
-
- Adetokunboh OO, Oluwasanu M. Eliminating mother-to-child transmission of the human immunodeficiency virus in sub-Saharan Africa: The journey so far and what remains to be done.Adetokunboh OO, Oluwasanu M. J Infect Public Health. 2016. Jul-Aug;9(4):396–407. doi: 10.1016/j.jiph.2015.06.010 - DOI - PubMed
-
- Mbizvo MT, Mmiro FA, Kasule J, Bagenda D, Mahomed K, Nathoo K, et al. Morbidity and mortality patterns in HIV-1 seropositive/ seronegative women in Kampala and Harare during pregnancy and in the subsequent two years. Cent Afr J Med 2005; 51(9–10): 91–7. - PubMed
-
- Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Nagalingeswaran K, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med 2011; 365(6): 493–505. doi: 10.1056/NEJMoa1105243 - DOI - PMC - PubMed
-
- Grinsztejn B, Hosseinipour MC, Ribaudo HJ, Swindells S, Eron J, Chen YG, et al. Effects of early versus delayed initiation of antiretroviral treatment on clinical outcomes of HIV-1 infection: results from the phase 3 HPTN 052 randomised controlled trial. Lancet Infect Dis 2014; 14(4): 281–90. doi: 10.1016/S1473-3099(13)70692-3 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
