

Cancer-Associated Mutations in Endometriosis without Cancer
- PMID: 28489996
- PMCID: PMC5555376
- DOI: 10.1056/NEJMoa1614814
Cancer-Associated Mutations in Endometriosis without Cancer
Abstract
Background: Endometriosis, defined as the presence of ectopic endometrial stroma and epithelium, affects approximately 10% of reproductive-age women and can cause pelvic pain and infertility. Endometriotic lesions are considered to be benign inflammatory lesions but have cancerlike features such as local invasion and resistance to apoptosis.
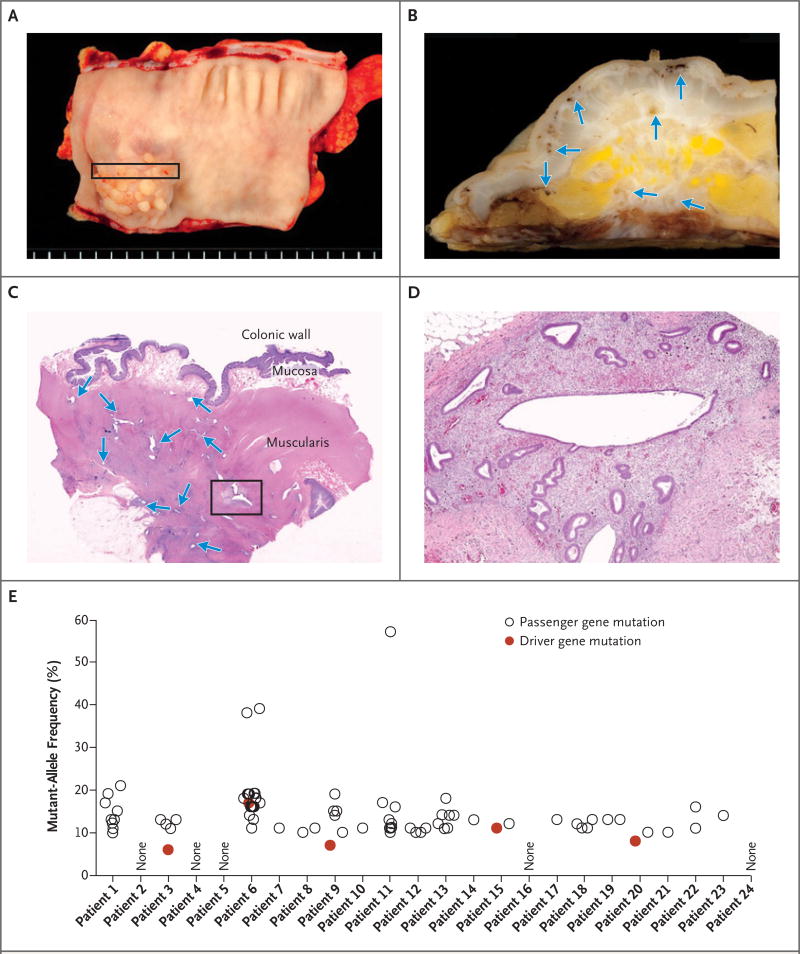
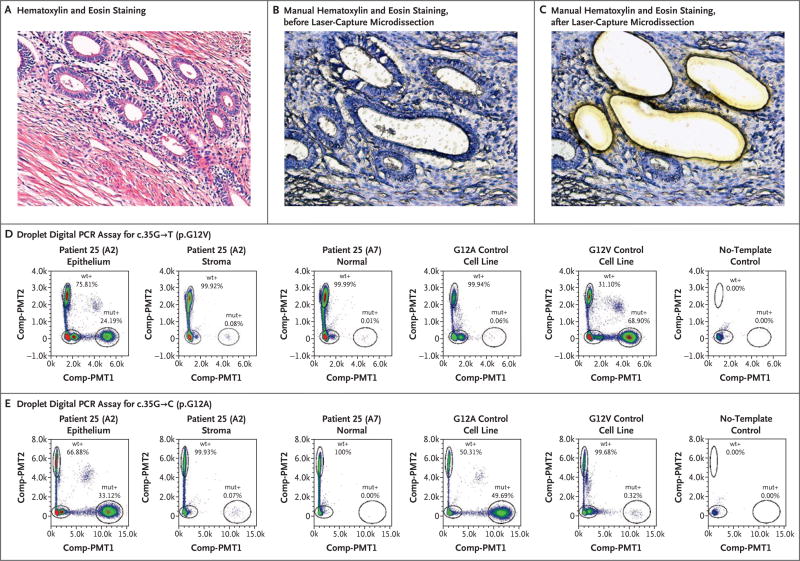
Methods: We analyzed deeply infiltrating endometriotic lesions from 27 patients by means of exomewide sequencing (24 patients) or cancer-driver targeted sequencing (3 patients). Mutations were validated with the use of digital genomic methods in microdissected epithelium and stroma. Epithelial and stromal components of lesions from an additional 12 patients were analyzed by means of a droplet digital polymerase-chain-reaction (PCR) assay for recurrent activating KRAS mutations.
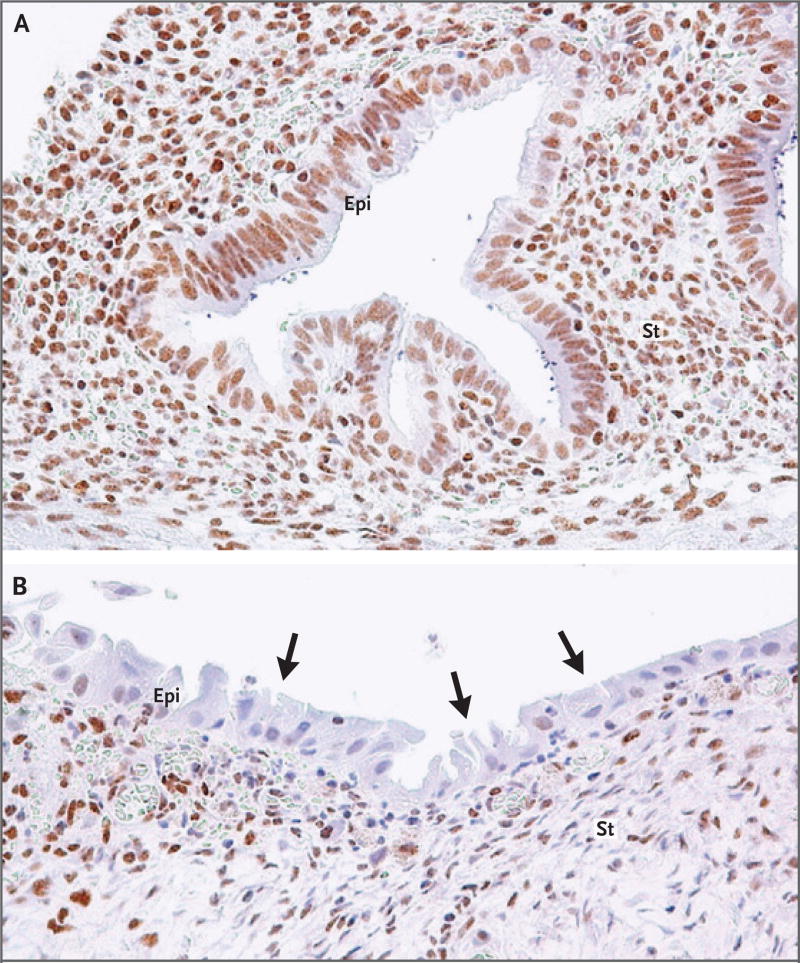
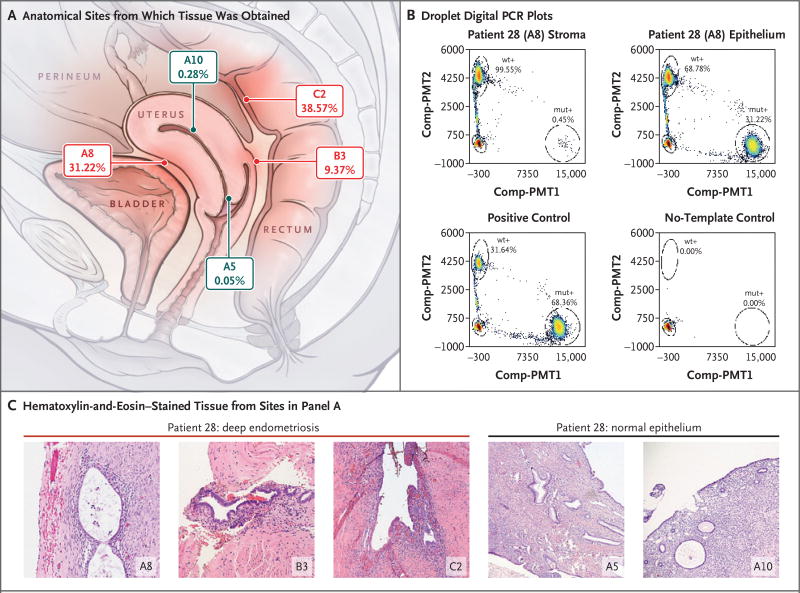
Results: Exome sequencing revealed somatic mutations in 19 of 24 patients (79%). Five patients harbored known cancer driver mutations in ARID1A, PIK3CA, KRAS, or PPP2R1A, which were validated by Safe-Sequencing System or immunohistochemical analysis. The likelihood of driver genes being affected at this rate in the absence of selection was estimated at P=0.001 (binomial test). Targeted sequencing and a droplet digital PCR assay identified KRAS mutations in 2 of 3 patients and 3 of 12 patients, respectively, with mutations in the epithelium but not the stroma. One patient harbored two different KRAS mutations, c.35G→T and c.35G→C, and another carried identical KRAS c.35G→A mutations in three distinct lesions.
Conclusions: We found that lesions in deep infiltrating endometriosis, which are associated with virtually no risk of malignant transformation, harbor somatic cancer driver mutations. Ten of 39 deep infiltrating lesions (26%) carried driver mutations; all the tested somatic mutations appeared to be confined to the epithelial compartment of endometriotic lesions.
Figures
Comment in
-
Driver mutations take the wheel in invasive yet nonmalignant disease.Sci Transl Med. 2017 Jun 7;9(393):eaan8194. doi: 10.1126/scitranslmed.aan8194. Sci Transl Med. 2017. PMID: 28592567
References
-
- Reese KA, Reddy S, Rock JA. Endometriosis in an adolescent population: the Emory experience. J Pediatr Adolesc Gynecol. 1996;9:125–8. - PubMed
-
- Bulun SE. Endometriosis. N Engl J Med. 2009;360:268–79. - PubMed
-
- Leyland N, Casper R, Laberge P, Singh SS. Endometriosis: diagnosis and management. J Obstet Gynaecol Can. 2010;32(Suppl 2):S1–S32. - PubMed
-
- Tosti C, Pinzauti S, Santulli P, Chapron C, Petraglia F. Pathogenetic mechanisms of deep infiltrating endometriosis. Reprod Sci. 2015;22:1053–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous