

Tumor necrosis factor inhibitors in psoriatic arthritis
- PMID: 28490202
- PMCID: PMC6348387
- DOI: 10.1080/17512433.2017.1329009
Tumor necrosis factor inhibitors in psoriatic arthritis
Abstract
Psoriatic arthritis (PsA) is a chronic inflammatory disease that can result in significant disability. With the emergence of tumor necrosis factor inhibitors (TNFi), therapeutic outcomes in PsA have improved substantially. The clinical efficacy and the inhibition of radiographic progression demonstrated by TNFi have transformed the management of PsA. However, there is still an unmet need for a subset of patients who do not respond adequately to TNFi. Areas covered: This review provides an overview of the pharmacokinetics of TNFi, the efficacy of TNFi in PsA, and the role of immunogenicity of TNFi in the treatment of PsA. In addition, we address the use of TNFi in the setting of other medications utilized in the treatment of PsA and the potential future role of biosimilars. Expert commentary: Monoclonal antibodies exhibit complex and widely variable pharmacokinetics. The study of factors that can affect the pharmacokinetics, such as immunogenicity, is valuable to further define and understand the use of TNFi in PsA, especially in the subset of patients who do not respond adequately to these agents or lose effectiveness over time.
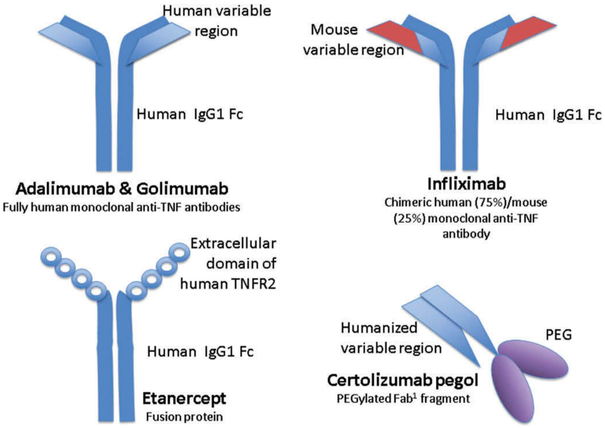
Keywords: Adalimumab; certolizumab; etanercept; golimumab; immunogenicity; infliximab; methotrexate; monoclonal antibodies; psoriatic arthritis; tumor necrosis factor inhibitors.
Figures
References
-
- Eder L, Gladman DD. Psoriatic arthritis: phenotypic variance and nosology. Curr Rheumatol Rep. 2013;15:316. - PubMed
-
- Ogdie A, Schwartzman S, Husni ME. Recognizing and managing comorbidities in psoriatic arthritis. Curr Opin Rheumatol. 2015. March;27(2):118–126. - PubMed
-
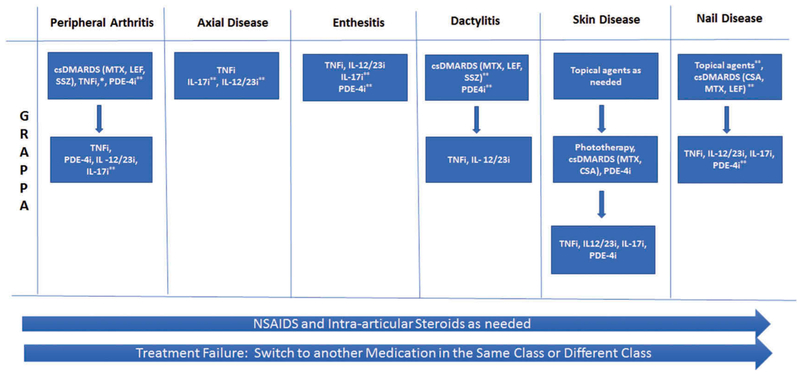
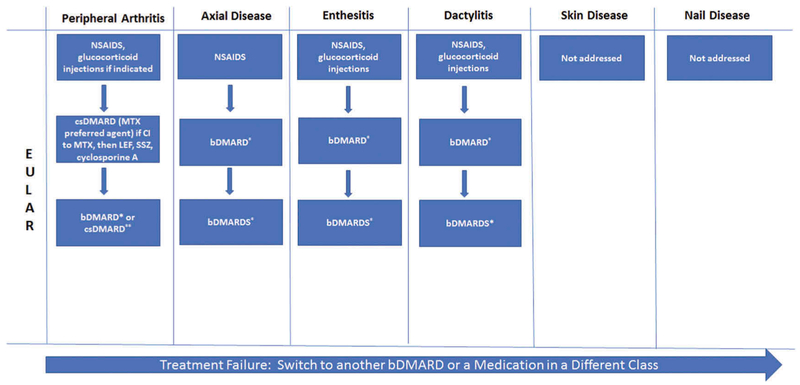
- Coates LC, Kavanaugh A, Mease PJ, et al. Group for research and assessment of psoriasis and psoriatic arthritis 2015 treatment recommendations for psoriatic arthritis. Arthritis Rheumatol. 2016;68(5):1060–1071. - PubMed
-
·· Treatment recommendations in psoriatic arthritis.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous