

Prevalence of Abnormal Magnetic Resonance Imaging Findings in Children with Persistent Symptoms after Pediatric Sports-Related Concussion
- PMID: 28490224
- PMCID: PMC5824661
- DOI: 10.1089/neu.2017.4970
Prevalence of Abnormal Magnetic Resonance Imaging Findings in Children with Persistent Symptoms after Pediatric Sports-Related Concussion
Abstract
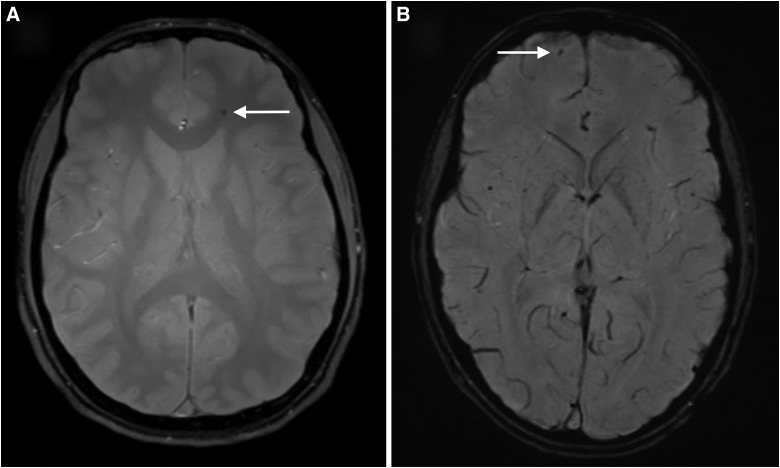
A subset of patients experience persistent symptoms after pediatric concussion, and magnetic resonance imaging (MRI) is commonly used to evaluate for pathology. The utility of this practice is unclear. We conducted a retrospective cohort study to describe the MRI findings in children with concussion. A registry of all patients seen at our institution from January 2010 through March 2016 with pediatric sports-related concussion was cross-referenced with a database of radiographical studies. Radiology reports were reviewed for abnormal findings. Patients with abnormal computed tomographies or MRI scans ordered for reasons other than concussion were excluded. Among 3338 children identified with concussion, 427 underwent MRI. Only 2 (0.5%) had findings compatible with traumatic injury, consisting in both of microhemorrhage. Sixty-one patients (14.3%) had abnormal findings unrelated to trauma, including 24 nonspecific T2 changes, 15 pineal cysts, eight Chiari I malformations, and five arachnoid cysts. One child underwent craniotomy for a cerebellar hemangioblastoma after presenting with ataxia; another had cortical dysplasia resected after seizure. The 2 patients with microhemorrhage each had three previous concussions, significantly more than patients whose scans were normal (median, 1) or abnormal without injury (median, 1.5; p = 0.048). MRI rarely revealed intracranial injuries in children post-concussion, and the clinical relevance of these uncommon findings remains unclear. Abnormalities unrelated to trauma are usually benign. However, MRI should be thoughtfully considered in children who present with concerning or atypical symptoms.
Keywords: brain concussion; magnetic resonance imaging; post-concussion syndrome.
Conflict of interest statement
R.H.B. received indirect salary support through an educational grant provided to the University of Washington Department of Neurological Surgery by Codman Neuro. S.R.B. has ownership in Aqueduct Neurosciences Inc, Aqueduct Critical Care Inc, and Navisonics Inc. C.L.M. has provided paid consulting services for Neurotrauma Sciences, LLC, and Sinapis Pharma, Inc. These commercial entities had no role in the design, conduct, or reporting of this research.
Figures
Similar articles
-
Neuroimaging findings in pediatric sports-related concussion.J Neurosurg Pediatr. 2015 Sep;16(3):241-7. doi: 10.3171/2015.1.PEDS14510. Epub 2015 Jun 2. J Neurosurg Pediatr. 2015. PMID: 26031620
-
Post-concussion syndrome (PCS) in a youth population: defining the diagnostic value and cost-utility of brain imaging.Childs Nerv Syst. 2015 Dec;31(12):2305-9. doi: 10.1007/s00381-015-2916-y. Epub 2015 Sep 29. Childs Nerv Syst. 2015. PMID: 26419243
-
Psychiatric outcomes after pediatric sports-related concussion.J Neurosurg Pediatr. 2015 Dec;16(6):709-18. doi: 10.3171/2015.5.PEDS15220. Epub 2015 Sep 11. J Neurosurg Pediatr. 2015. PMID: 26359916
-
[Mild traumatic brain injury and postconcussive syndrome: a re-emergent questioning].Encephale. 2012 Sep;38(4):329-35. doi: 10.1016/j.encep.2011.07.003. Epub 2011 Aug 31. Encephale. 2012. PMID: 22980474 Review. French.
-
Diagnosis of concussion: the role of imaging now and in the future.Phys Med Rehabil Clin N Am. 2011 Nov;22(4):635-52, viii. doi: 10.1016/j.pmr.2011.08.005. Epub 2011 Sep 25. Phys Med Rehabil Clin N Am. 2011. PMID: 22050940 Review.
Cited by
-
Clinical Assessment of Concussion and Persistent Post-Concussive Symptoms for Neurologists.Curr Neurol Neurosci Rep. 2021 Nov 24;21(12):70. doi: 10.1007/s11910-021-01159-2. Curr Neurol Neurosci Rep. 2021. PMID: 34817724 Review.
-
Neuroaudiological Considerations for the Auditory Brainstem Response and Middle Latency Response Revisited: Back to the Future.Semin Hear. 2022 Oct 26;43(3):149-161. doi: 10.1055/s-0042-1756161. eCollection 2022 Aug. Semin Hear. 2022. PMID: 36313049 Free PMC article. Review.
-
No Evidence of a Difference in Susceptibility-Weighted Imaging Lesion Burden or Functional Network Connectivity between Children with Typical and Delayed Recovery Two Weeks Post-Concussion.J Neurotrauma. 2021 Sep 1;38(17):2384-2390. doi: 10.1089/neu.2021.0069. Epub 2021 Jul 30. J Neurotrauma. 2021. PMID: 33823646 Free PMC article.
-
Post-Traumatic Headache in Children after Minor Head Trauma: Incidence, Phenotypes, and Risk Factors.Children (Basel). 2023 Mar 10;10(3):534. doi: 10.3390/children10030534. Children (Basel). 2023. PMID: 36980092 Free PMC article.
-
Prevalence of Potentially Clinically Significant Magnetic Resonance Imaging Findings in Athletes with and without Sport-Related Concussion.J Neurotrauma. 2019 Jun;36(11):1776-1785. doi: 10.1089/neu.2018.6055. Epub 2019 Feb 25. J Neurotrauma. 2019. PMID: 30618331 Free PMC article.
References
-
- Bryan M.A., Rowhani-Rahbar A., Comstock R.D., and Rivara F.; Seattle Sports Concussion Research Collaborative. (2016). Sports- and recreation-related concussions in US youth. Pediatrics 138, e20154635–e20154635 - PubMed
-
- McCrory P., Meeuwisse W.H., Aubry M., Cantu B., Dvorák J., Echemendia R.J., Engebretsen L., Johnston K., Kutcher J.S., Raftery M., Sills A., Benson B.W., Davis G.A., Ellenbogen R.G., Guskiewicz K., Herring S.A., Iverson G.L., Jordan B.D., Kissick J., McCrea M., McIntosh A.S., Maddocks D., Makdissi M., Purcell L., Putukian M., Schneider K., Tator C.H., and Turner M. (2013). Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br. J. Sports Med. 47, 250–258 - PubMed
-
- Zemek R., Barrowman N., Freedman S.B., Gravel J., Gagnon I., McGahern C., Aglipay M., Sangha G., Boutis K., Beer D., Craig W., Burns E., Farion K.J., Mikrogianakis A., Barlow K., Dubrovsky A.S., Meeuwisse W., Gioia G., Meehan W.P., Beauchamp M.H., Kamil Y., Grool A.M., Hoshizaki B., Anderson P., Brooks B.L., Yeates K.O., Vassilyadi M., Klassen T., Keightley M., Richer L., DeMatteo C., and Osmond M.H.; Pediatric Emergency Research Canada (PERC) Concussion Team. (2016). Clinical risk score for persistent postconcussion symptoms among children with acute concussion in the ED. JAMA 315, 1014–1025 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
