

Longitudinal Associations among Renal Urea Clearance-Corrected Normalized Protein Catabolic Rate, Serum Albumin, and Mortality in Patients on Hemodialysis
- PMID: 28490436
- PMCID: PMC5498364
- DOI: 10.2215/CJN.13141216
Longitudinal Associations among Renal Urea Clearance-Corrected Normalized Protein Catabolic Rate, Serum Albumin, and Mortality in Patients on Hemodialysis
Abstract
Background and objectives: There are inconsistent reports on the association of dietary protein intake with serum albumin and outcomes among patients on hemodialysis. Using a new normalized protein catabolic rate (nPCR) variable accounting for residual renal urea clearance, we hypothesized that higher baseline nPCR and rise in nPCR would be associated with higher serum albumin and better survival among incident hemodialysis patients.
Design, setting, participants, & measurements: Among 36,757 incident hemodialysis patients in a large United States dialysis organization, we examined baseline and change in renal urea clearance-corrected nPCR as a protein intake surrogate and modeled their associations with serum albumin and mortality over 5 years (1/2007-12/2011).
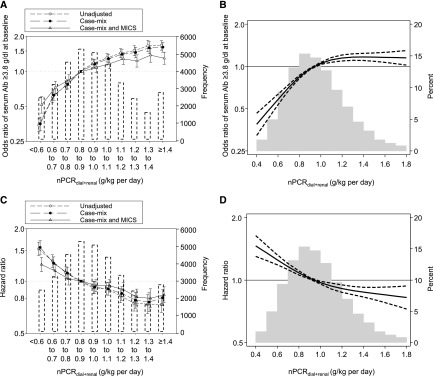
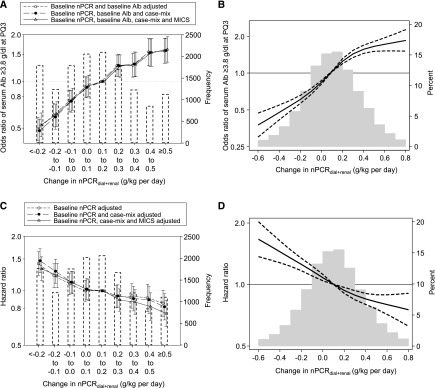
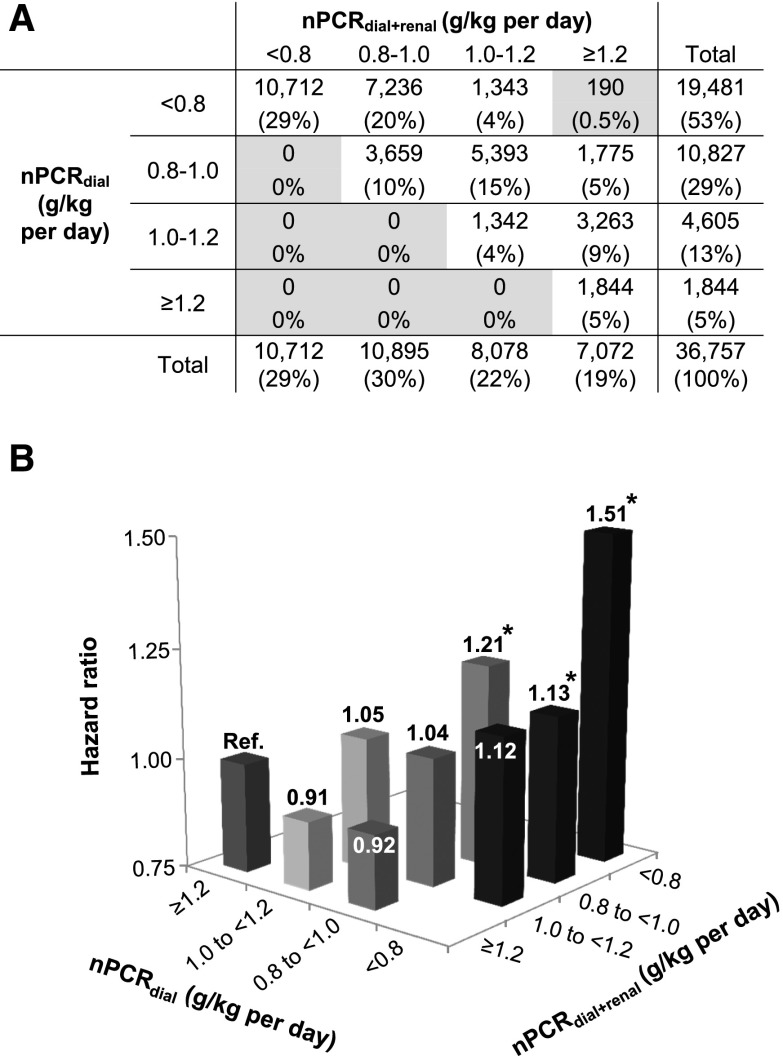
Results: Median nPCRs with and without accounting for renal urea clearance at baseline were 0.94 and 0.78 g/kg per day, respectively (median within-patient difference, 0.14 [interquartile range, 0.07-0.23] g/kg per day). During a median follow-up period of 1.4 years, 8481 deaths were observed. Baseline renal urea clearance-corrected nPCR was associated with higher serum albumin and lower mortality in the fully adjusted model (Ptrend<0.001). Among 13,895 patients with available data, greater rise in renal urea clearance-corrected nPCR during the first 6 months was also associated with attaining high serum albumin (≥3.8 g/dl) and lower mortality (Ptrend<0.001); compared with the reference group (a change of 0.1-0.2 g/kg per day), odds and hazard ratios were 0.53 (95% confidence interval, 0.44 to 0.63) and 1.32 (95% confidence interval, 1.14 to 1.54), respectively, among patients with a change of <-0.2 g/kg per day and 1.62 (95% confidence interval, 1.35 to 1.96) and 0.76 (95% confidence interval, 0.64 to 0.90), respectively, among those with a change of ≥0.5 g/kg per day. Within a given category of nPCR without accounting for renal urea clearance, higher levels of renal urea clearance-corrected nPCR consistently showed lower mortality risk.
Conclusions: Among incident hemodialysis patients, higher dietary protein intake represented by nPCR and its changes over time appear to be associated with increased serum albumin levels and greater survival. nPCR may be underestimated when not accounting for renal urea clearance. Compared with the conventional nPCR, renal urea clearance-corrected nPCR may be a better marker of mortality.
Keywords: Dietary Proteins; Dietary protein intake (DPI); Fluid Therapy; Follow-Up Studies; Humans; Odds Ratio; Proportional Hazards Models; Serum Albumin; Urinary Tract Physiological Phenomena; albumin; hemodialysis; mortality; protein catabolic rate (PCR); renal dialysis; residual kidney function; urea.
Copyright © 2017 by the American Society of Nephrology.
Figures

References
-
- Kalantar-Zadeh K, Kopple JD, Block G, Humphreys MH: A malnutrition-inflammation score is correlated with morbidity and mortality in maintenance hemodialysis patients. Am J Kidney Dis 38: 1251–1263, 2001 - PubMed
-
- Kalantar-Zadeh K, Kilpatrick RD, Kuwae N, McAllister CJ, Alcorn H Jr., Kopple JD, Greenland S: Revisiting mortality predictability of serum albumin in the dialysis population: Time dependency, longitudinal changes and population-attributable fraction. Nephrol Dial Transplant 20: 1880–1888, 2005 - PubMed
-
- Fouque D, Kalantar-Zadeh K, Kopple J, Cano N, Chauveau P, Cuppari L, Franch H, Guarnieri G, Ikizler TA, Kaysen G, Lindholm B, Massy Z, Mitch W, Pineda E, Stenvinkel P, Treviño-Becerra A, Wanner C: A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int 73: 391–398, 2008 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
