

Perioperative COX-2 and β-Adrenergic Blockade Improves Metastatic Biomarkers in Breast Cancer Patients in a Phase-II Randomized Trial
- PMID: 28490464
- PMCID: PMC5559335
- DOI: 10.1158/1078-0432.CCR-17-0152
Perioperative COX-2 and β-Adrenergic Blockade Improves Metastatic Biomarkers in Breast Cancer Patients in a Phase-II Randomized Trial
Abstract
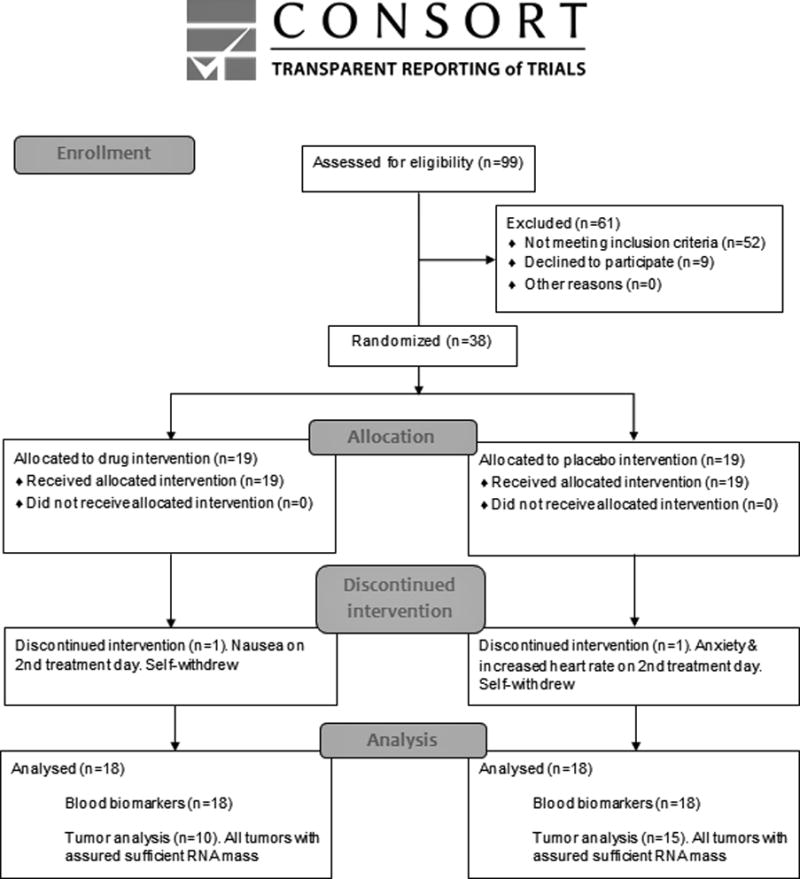
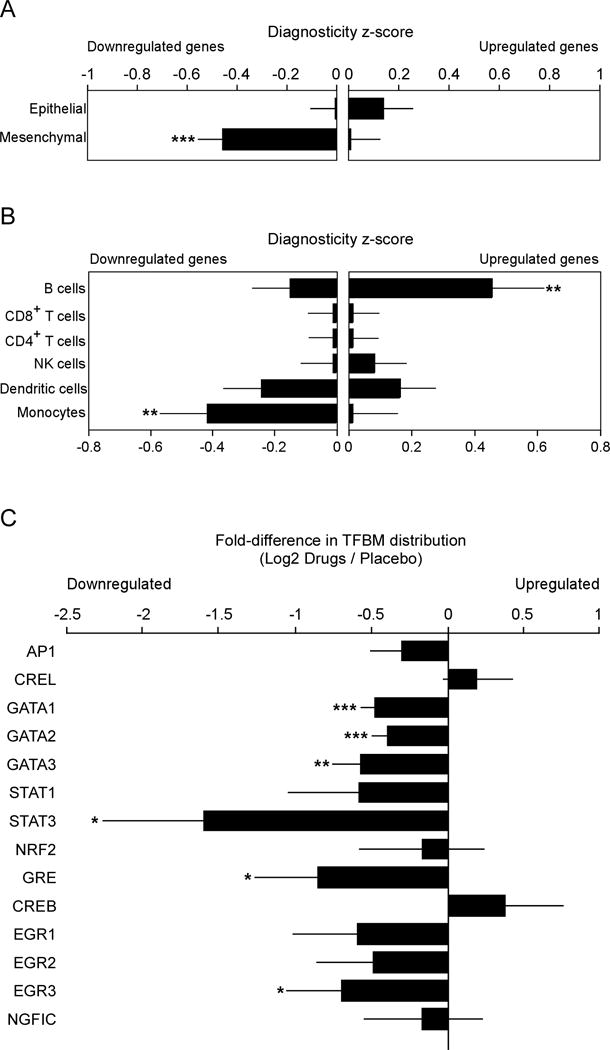
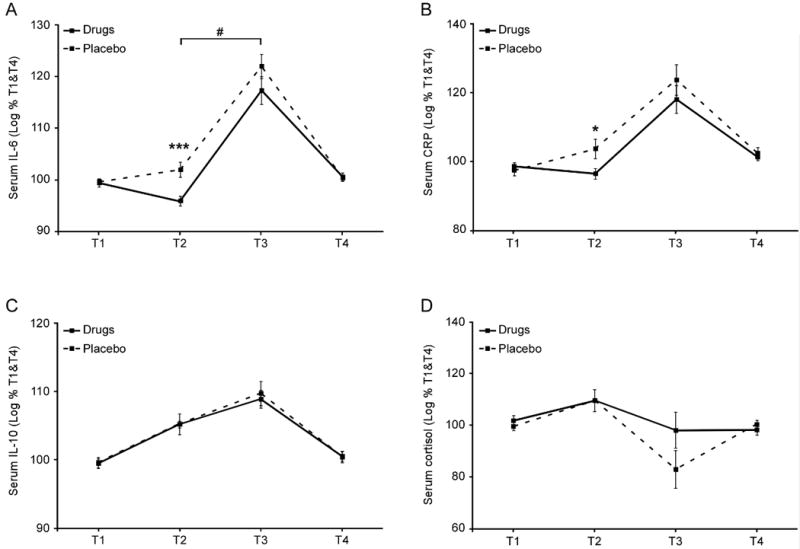
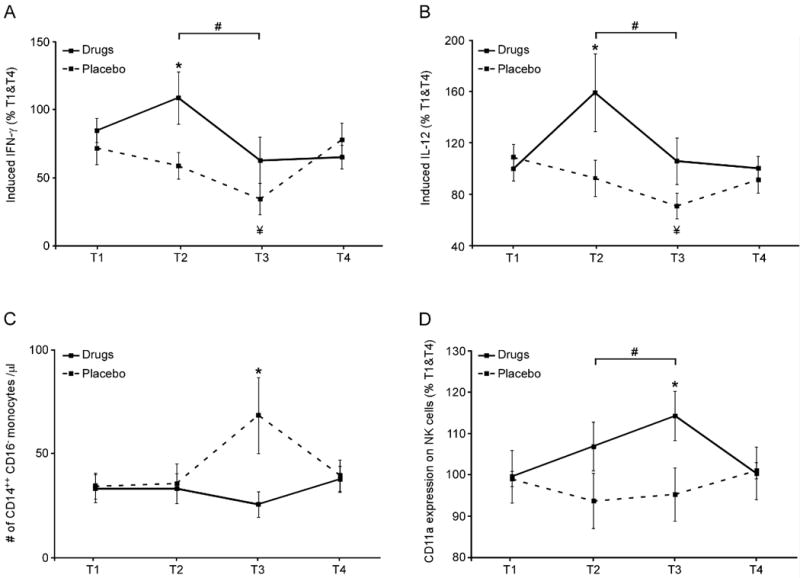
Purpose: Translational studies suggest that excess perioperative release of catecholamines and prostaglandins may facilitate metastasis and reduce disease-free survival. This trial tested the combined perioperative blockade of these pathways in breast cancer patients.Experimental Design: In a randomized placebo-controlled biomarker trial, 38 early-stage breast cancer patients received 11 days of perioperative treatment with a β-adrenergic antagonist (propranolol) and a COX-2 inhibitor (etodolac), beginning 5 days before surgery. Excised tumors and sequential blood samples were assessed for prometastatic biomarkers.Results: Drugs were well tolerated with adverse event rates comparable with placebo. Transcriptome profiling of the primary tumor tested a priori hypotheses and indicated that drug treatment significantly (i) decreased epithelial-to-mesenchymal transition, (ii) reduced activity of prometastatic/proinflammatory transcription factors (GATA-1, GATA-2, early-growth-response-3/EGR3, signal transducer and activator of transcription-3/STAT-3), and (iii) decreased tumor-infiltrating monocytes while increasing tumor-infiltrating B cells. Drug treatment also significantly abrogated presurgical increases in serum IL6 and C-reactive protein levels, abrogated perioperative declines in stimulated IL12 and IFNγ production, abrogated postoperative mobilization of CD16- "classical" monocytes, and enhanced expression of CD11a on circulating natural killer cells.Conclusions: Perioperative inhibition of COX-2 and β-adrenergic signaling provides a safe and effective strategy for inhibiting multiple cellular and molecular pathways related to metastasis and disease recurrence in early-stage breast cancer. Clin Cancer Res; 23(16); 4651-61. ©2017 AACR.
©2017 American Association for Cancer Research.
Conflict of interest statement
Disclosures provided by the authors are available with this article at
Figures

References
-
- Shakhar G, Ben-Eliyahu S. Potential prophylactic measures against postoperative immunosuppression: could they reduce recurrence rates in oncological patients? Annals of surgical oncology. 2003;10(8):972–92. - PubMed
-
- Armaiz-Pena GN, Gonzalez-Villasana V, Nagaraja AS, Rodriguez-Aguayo C, Sadaoui NC, Stone RL, et al. Adrenergic regulation of monocyte chemotactic protein 1 leads to enhanced macrophage recruitment and ovarian carcinoma growth. Oncotarget. 2015;6(6):4266–73. doi: 10.18632/oncotarget.2887. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
