

Universal molecular screening does not effectively detect Lynch syndrome in clinical practice
- PMID: 28491141
- PMCID: PMC5405883
- DOI: 10.1177/1756283X17690990
Universal molecular screening does not effectively detect Lynch syndrome in clinical practice
Abstract
Background: Lynch syndrome (LS) due to an inherited damaging mutation in mismatch repair (MMR) genes comprises 3% of all incident colorectal cancer (CRC). Molecular testing using immunohistochemistry (IHC) for MMR proteins is a recommended screening tool to identify LS in incident CRC. This study assessed outcomes of population-based routine molecular screening for diagnosis of LS in a regional center.
Methods: We conducted a prospective, consecutive case series study of universal IHC testing on cases of resected CRC from September 2004-December 2013. Referred cases with abnormal IHC results that attended a familial cancer clinic were assessed according to modified Bethesda criteria (until 2009) or molecular criteria (from 2009).
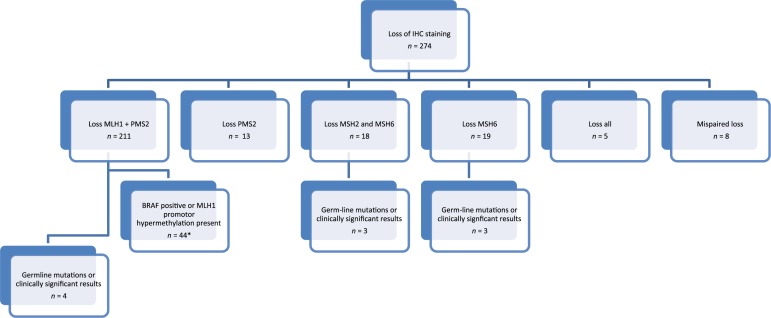
Results: 1612 individuals underwent resection for CRC in the study period and had MMR testing by IHC. Of these, 274 cases (16.9%) exhibited loss of expression of MMR genes. The mean age at CRC diagnosis was 68.1 years (± standard deviation 12.7) and the mean age of those with an IHC abnormality was 71.6 (± 11.8). A total of 82 (29.9%) patients with an abnormal result were seen in a subspecialty familial cancer clinic. Patients aged under 50 (p = 0.009) and those with loss of MSH6 staining (p = 0.027) were more likely to be referred and to attend. After germ-line sequencing, 0.6% (10 of 82) were identified as having a clinically significant abnormality. A further eight probands with pathogenic germ-line mutations were identified from other referrals to the service over the same time period.
Conclusions: While technically accurate, the yield of 'universal' IHC in detecting new Lynch probands is limited by real-world factors that reduce referrals and genetic testing. We propose an alternative approach for universal, incident case detection of Lynch syndrome with 'one-stop' MMR testing and sequencing.
Keywords: DNA mismatch repair; Lynch syndrome; colorectal neoplasms; immunohistochemistry.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
Figures
References
-
- Hampel H, Frankel WL, Martin E, et al. Screening for the Lynch syndrome (hereditary nonpolyposis colorectal cancer). N Engl J Med 2005; 352: 1851–1860. - PubMed
-
- Lung MS, Trainer AH, Campbell I, et al. Familial colorectal cancer. Intern Med J 2015; 45: 482–491. - PubMed
-
- Bonadona V, Bonaïti B, Olschwang S, et al. Cancer risks associated with germline mutations in MLH1, MSH2, and MSH6 genes in Lynch syndrome. JAMA 2011; 305: 2304–2310. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
