

Clinical effectiveness and toxicity of second-line irinotecan in advanced gastric and gastroesophageal junction adenocarcinoma: a single-center observational study
- PMID: 28491144
- PMCID: PMC5405997
- DOI: 10.1177/1758834016689029
Clinical effectiveness and toxicity of second-line irinotecan in advanced gastric and gastroesophageal junction adenocarcinoma: a single-center observational study
Abstract
Background: Randomized clinical trials showed improved overall survival (OS) of advanced gastroesophageal adenocarcinoma (GEA) patients treated with second-line taxane or irinotecan. However, most data on irinotecan efficacy in this setting come from large Asian trials. We retrospectively analyzed clinical effectiveness and toxicity of irinotecan in a cohort of patients with advanced GEA treated in our department.
Methods: Advanced GEA patients who received at least one cycle of second-line irinotecan were eligible for inclusion. Irinotecan was administered every 3 weeks at an initial dose of 250 mg/m2 of body surface area with subsequent gradual (every 50 mg/m2) dose escalation up to 350 mg/m2, in the case of good treatment tolerance. OS was estimated using the Kaplan-Meier method. A multivariate Cox regression analysis was used to examine the association between clinical and laboratory parameters and survival.
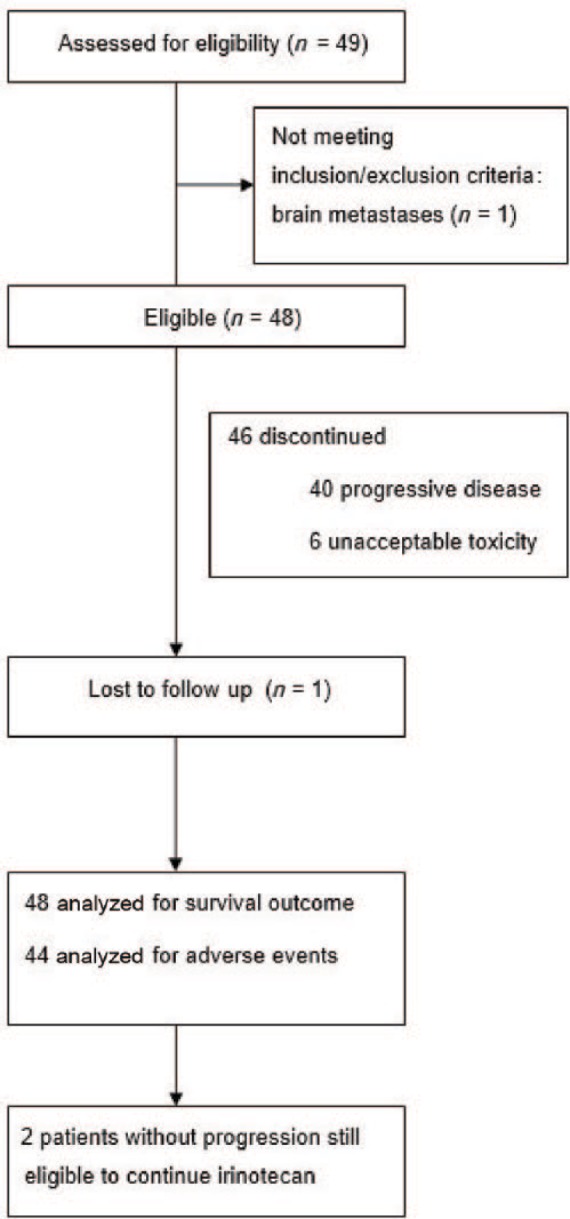
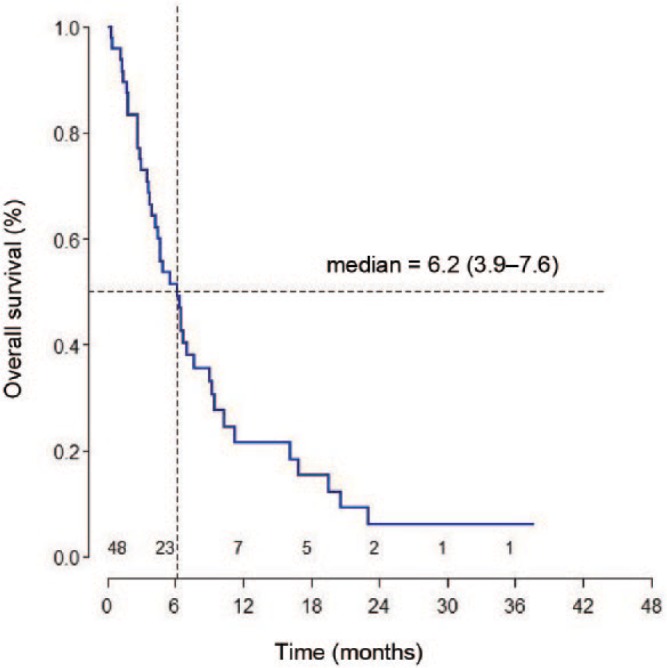
Results: A total of 48 patients were identified. Median OS was 6.2 months [95% confidence interval (CI): 3.9-7.6]. In multivariate analysis, age < 65 years, baseline total lymphocyte count (TLC) < 1500/µl and presence of peritoneal metastases were associated with shorter OS. Most adverse events were grade 1-2 and included: anemia (52.3%), leukocytopenia (40.9%), neutropenia (59.1%), nausea (25.0%), vomiting (31.8%), diarrhea (31.8%), anorexia (29.5%) and fatigue (43.2%). Febrile neutropenia occurred in three patients (6.8%). Nine patients (20.5%) experienced a toxicity grade 3-4 of any kind.
Conclusions: This retrospective analysis confirms clinical effectiveness and manageable toxicity of second-line irinotecan in an unselected cohort of advanced GEA patients. Age < 65 years, baseline TLC < 1500/µl and presence of peritoneal metastases were independent prognostic factors associated with shorter OS.
Keywords: gastric cancer; gastroesophageal cancer; irinotecan; second-line chemotherapy.
Conflict of interest statement
Conflict of interest statement: Dr. Ochenduszko received speaker honoraria from Roche, Amgen and Lilly and received financial support for attending symposia from Roche, Janssen and Pfizer. All other authors declare that they have no conflicts of interest.
Figures
References
-
- Andreyev H., Norman A., Oates J., Cunningham D. (1998) Why do patients with weight loss have a worse outcome when undergoing chemotherapy for gastrointestinal malignancies? Eur J Cancer 34: 503–509. - PubMed
-
- Chau I., Ashley S., Cunningham D. (2009) Validation of the Royal Marsden Hospital prognostic index in advanced esophagogastric cancer using individual patient data from the REAL 2 study. J Clin Oncol 27: 3–4. - PubMed
-
- Chau I., Norman A., Cunningham D., Waters J., Oates J., Ross P. (2004) Multivariate prognostic factor analysis in locally advanced and metastatic esophago-gastric cancer - pooled analysis from three multicenter, randomized, controlled trials using individual patient data. J Clin Oncol 22: 2395–2403. - PubMed
-
- Dreyer N., Tunis S., Berger M., Ollendorf D., Mattox P., Gliklich R. (2010) Why observational studies should be among the tools used in comparative effectiveness research. Health Aff 29: 1818–1825. - PubMed
-
- Ford H., Marshall A., Bridgewater J., Janowitz T., Coxon F., Wadsley J., et al. (2014) Docetaxel versus active symptom control for refractory oesophagogastric adenocarcinoma (COUGAR-02): an open-label, phase 3 randomised controlled trial. Lancet Oncol 15: 78–86. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
