

The Clinical Epidemiology and 30-Day Outcomes of Emergency Department Patients With Acute Kidney Injury
- PMID: 28491339
- PMCID: PMC5406199
- DOI: 10.1177/2054358117703985
The Clinical Epidemiology and 30-Day Outcomes of Emergency Department Patients With Acute Kidney Injury
Abstract
Background: Acute kidney injury (AKI) is associated with increased mortality and dialysis in hospitalized patients but has been little explored in the emergency department (ED) setting.
Objective: The objective of this study was to describe the risk factors, prevalence, management, and outcomes in the ED population, and to identify the proportion of AKI patients who were discharged home with no renal-specific follow-up.
Design: This is a retrospective cohort study using administrative and laboratory databases.
Setting: Two urban EDs in Vancouver, British Columbia, Canada.
Patients: We included all unique ED patients over a 1-week period.
Methods: All patients had their described demographics, comorbidities, medications, laboratory values, and ED treatments collected. AKI was defined pragmatically, based upon accepted guidelines. The cohort was then probabilistically linked to the provincial renal database to ascertain renal replacement (transplant or dialysis) and the provincial vital statistics database to obtain mortality. The primary outcome was the prevalence of AKI; secondary outcomes included (1) the proportion of AKI patients who were discharged home with no renal-specific follow-up and (2) the combined 30-day rate of death or renal replacement among AKI patients.
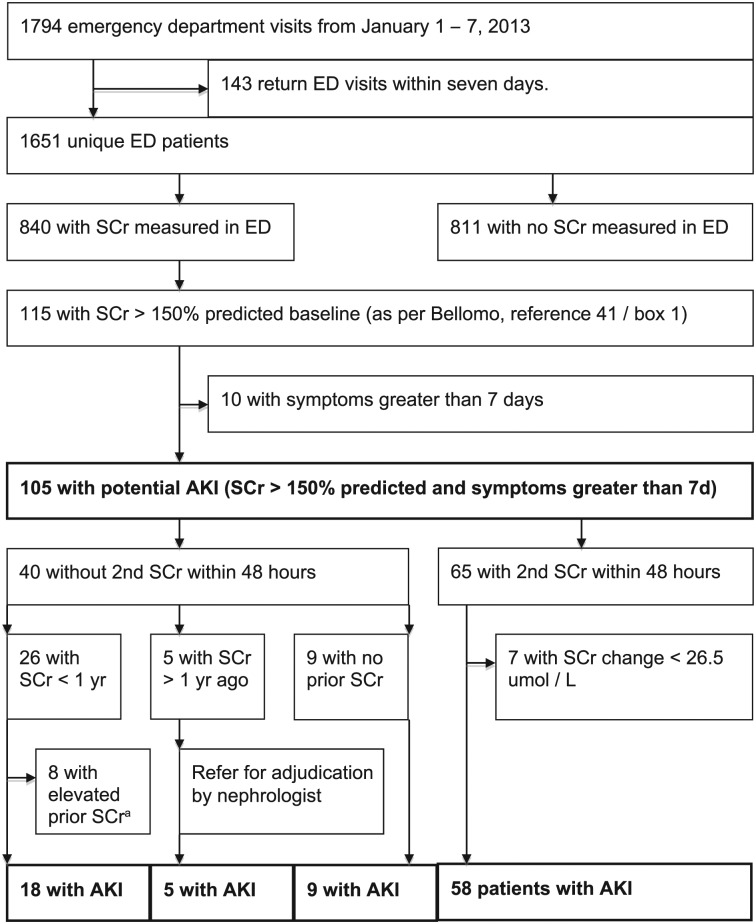
Results: There were 1651 ED unique patients, and 840 had at least one serum creatinine (SCr) obtained. Overall, 90 patients had AKI (10.7% of ED patients with at least one SCr, 95% confidence interval [CI], 8.7%-13.1%; 5.5% of all ED patients, 95% CI, 4.4%-6.7%) with a median age of 74 and 70% male. Of the 31 (34.4%) AKI patients discharged home, 4 (12.9%) had renal-specific follow-up arranged in the ED. Among the 90 AKI patients, 11 died and none required renal replacement at 30 days, for a combined outcome of 12.2% (95% CI, 6.5%-21.2%).
Limitations: Sample sizes may be small. Nearly half of ED patients did not obtain an SCr. Many patients did not have sequential SCr testing, and a modified definition of AKI was used.
Mise en contexte: L’insuffisance rénale aiguë (IRA) est associée à une mortalité accrue et à un recours plus fréquent à l’hémodialyse chez les patients hospitalisés. Toutefois, l’IRA a très peu été étudiée dans le cadre du service des urgences.
Objectif de l’étude: Dresser le portrait des facteurs de risque, de la prévalence, de la prise en charge et des conséquences de l’IRA au sein d’une population de patients admis aux urgences. Établir la proportion de patients atteints d’IRA qui ont par la suite été renvoyés à la maison sans aucun suivi en néphrologie.
Modèle d’étude: Il s’agit d’une étude de cohorte rétrospective menée à partir des bases de données administratives et de laboratoire des hôpitaux concernés.
Cadre de l’étude: L’étude s’est tenue dans deux services d’urgence de Vancouver (CB) au Canada.
Participants: Nous avons inclus tous les patients ayant été admis aux urgences au cours d’une période d’une semaine.
Méthodologie: Les données démographiques, les comorbidités, la liste des médicaments prescrits, les résultats de laboratoire et les traitements administrés lors du séjour aux urgences ont été colligés pour chacun des participants. L’IRA a été définie avec pragmatisme, conformément aux lignes directrices acceptées. La cohorte a ensuite été couplée de façon probabiliste à la base de données provinciale sur l’insuffisance rénale afin d’évaluer l’incidence de thérapies de remplacement rénal (dialyse ou greffe) et la base de données statistique provinciale pour obtenir le taux de mortalité. Le critère de jugement principal était la prévalence de l’IRA ; les critères de jugement secondaires incluaient la proportion de patients atteints d’IRA retournés à la maison sans prescription de suivi en santé rénale ainsi que le taux combiné de mortalité ou d’établissement d’une thérapie de remplacement rénal à l’intérieur de 30 jours chez ces mêmes patients.
Résultats: Au total, 1 651 patients se sont présentés aux urgences au cours de la période étudiée. Au moins une mesure de la créatinine sérique (SCr) avait été effectuée pour 840 d’entre eux. Dans l’ensemble, 90 patients souffraient effectivement d’IRA, (10,7% des patients avec au moins une mesure de SCr [IC à 95%: 8,7 à 13,1%] ; 5,5% de tous les patients [IC à 95%: 4,4 à 6,7%]). Il s’agissait de patients majoritairement de sexe masculin (70%) et leur âge médian était de 74 ans. Des 31 patients souffrant d’IRA (34,4%) retournés à la maison, on a prévu un suivi en santé rénale pour seulement quatre (12,9%) d’entre eux pendant leur séjour aux urgences. Parmi les 90 patients souffrant d’IRA, 11 sont décédés et aucun n’a eu besoin d’une thérapie de remplacement de la fonction rénale dans les 30 jours suivant la visite aux urgences, ce qui représente un résultat combiné de 12,2% (IC à 95%: 6,5 à 21,2%).
Limites de l’étude: Le faible échantillonnage et le fait qu’aucune mesure de la SCr n’ait été effectuée pour près de la moitié des patients ayant séjourné aux urgences. De plus, plusieurs patients pour qui on avait procédé à une mesure de la SCr n’ont pas eu de mesure séquentielle, et une définition modifiée de l’insuffisance rénale a été utilisée pour réaliser l’étude.
Keywords: acute kidney injury; outcomes.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Comment in
-
Emergency Department Patients With Acute Kidney Injury: Appropriately Discharged but Inadequately Followed-Up?Acad Emerg Med. 2018 Jul;25(7):815-818. doi: 10.1111/acem.13379. Epub 2018 Feb 15. Acad Emerg Med. 2018. PMID: 29360211 No abstract available.
References
-
- Levin A, Warnock DG, Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C. Improving outcomes from acute kidney injury: report of an initiative. Am J Kidney Dis. 2007;50:1-4. - PubMed
-
- Kellum JA, Bellomo R, Ronco C, Mehta R, Clark W, Levin NW. The 3rd international consensus conference of the acute dialysis quality initiative (ADQI). Int J Artif Organs 2005;28:441-444. - PubMed
-
- Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39:930-936. - PubMed
-
- Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294:813-818. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
