

Screening of conventional anticonvulsants in a genetic mouse model of epilepsy
- PMID: 28491900
- PMCID: PMC5420810
- DOI: 10.1002/acn3.413
Screening of conventional anticonvulsants in a genetic mouse model of epilepsy
Abstract
Objective: Epilepsy is a common neurological disorder that affects 1% of the population. Approximately, 30% of individuals with epilepsy are refractory to treatment, highlighting the need for novel therapies. Conventional anticonvulsant screening relies predominantly on induced seizure models. However, these models may not be etiologically relevant for genetic epilepsies. Mutations in SCN1A are a common cause of Dravet Syndrome, a severe epileptic encephalopathy. Dravet syndrome typically begins in infancy with seizures provoked by fever and then progresses to include afebrile pleomorphic seizure types. Affected children respond poorly to available anticonvulsants. Scn1a+/- heterozygous knockout mice recapitulate features of Dravet syndrome and provide a potential screening platform to investigate novel therapeutics. In this study, we conducted a screening of conventional anticonvulsants in Scn1a+/- mice to establish assays that most closely correlate with human response data.
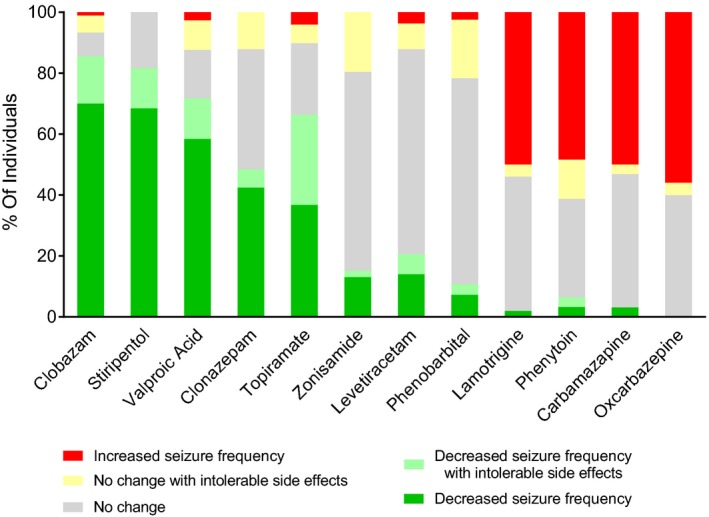
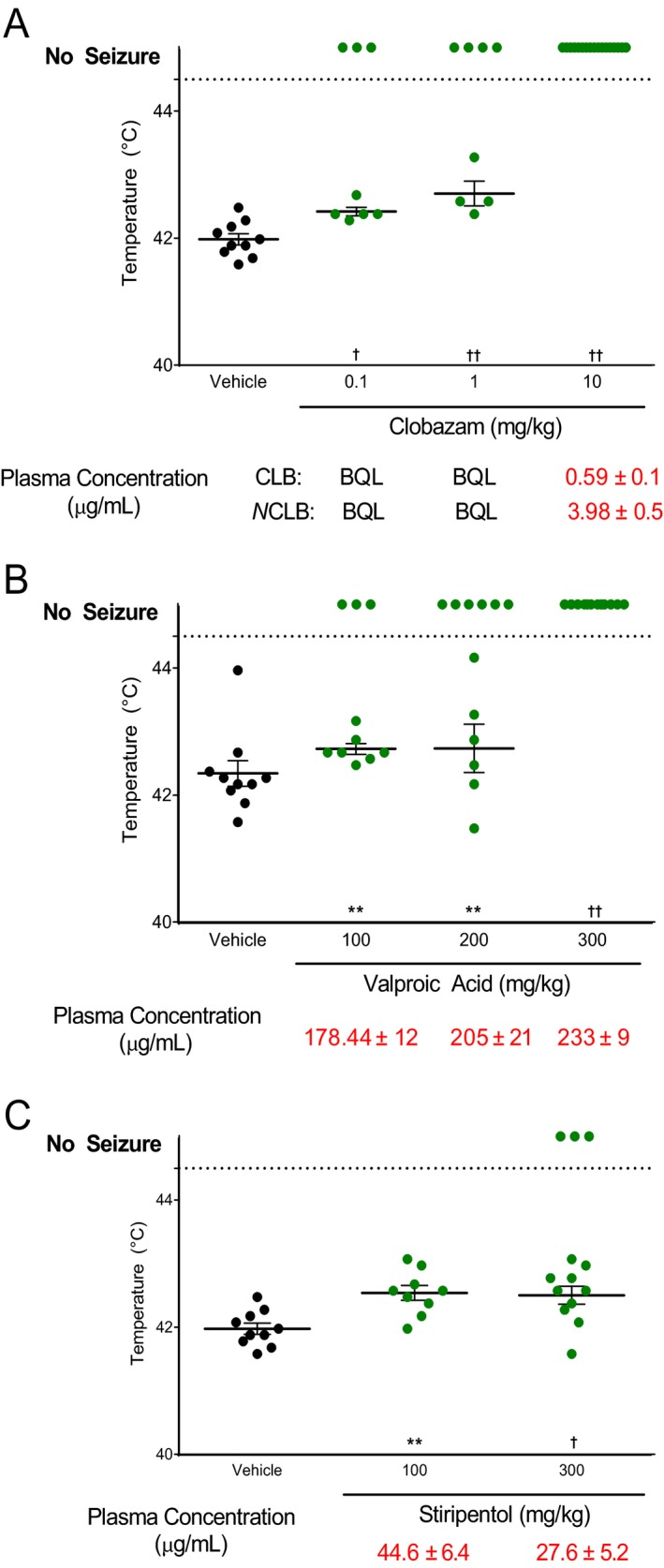
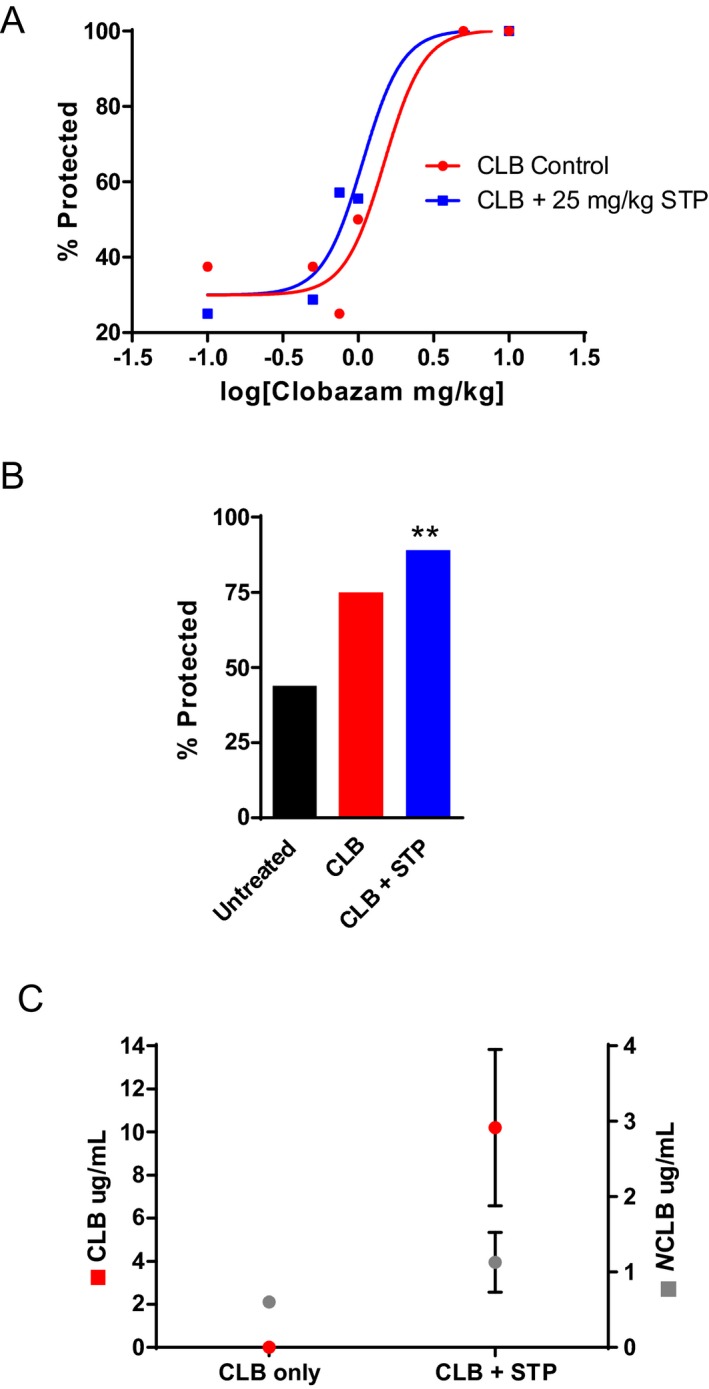
Methods: On the basis of clinical response data from a large, single center, retrospective survey of Dravet syndrome case records, we selected nine drugs for screening in Scn1a+/- mice to determine which phenotypic measures correlate best with human therapeutic response. We evaluated several screening paradigms and incorporated pharmacokinetic monitoring to establish drug exposure levels.
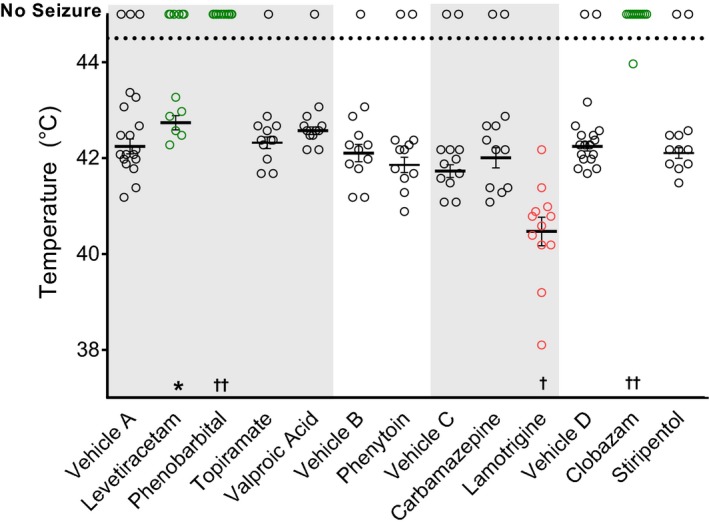
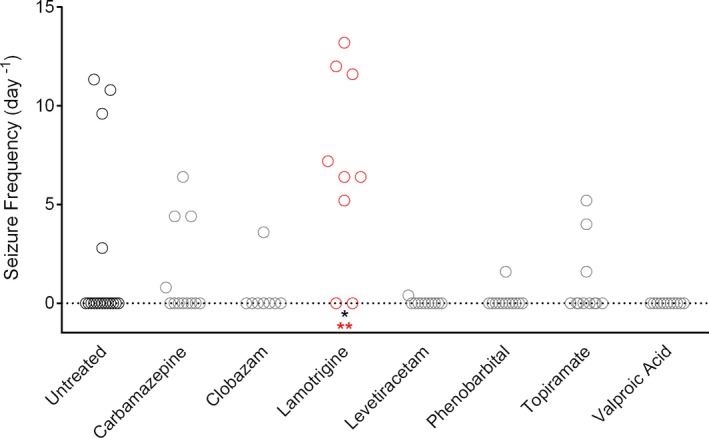
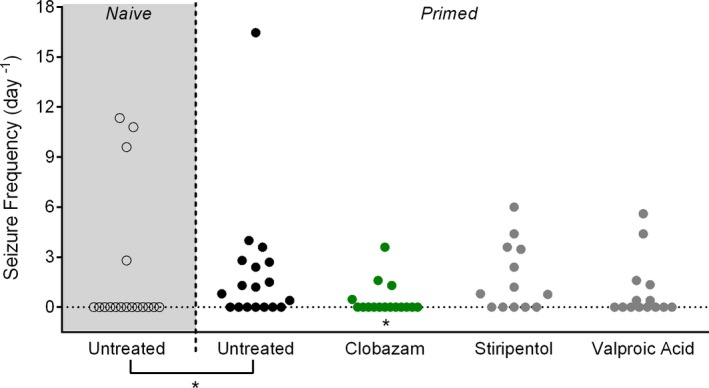
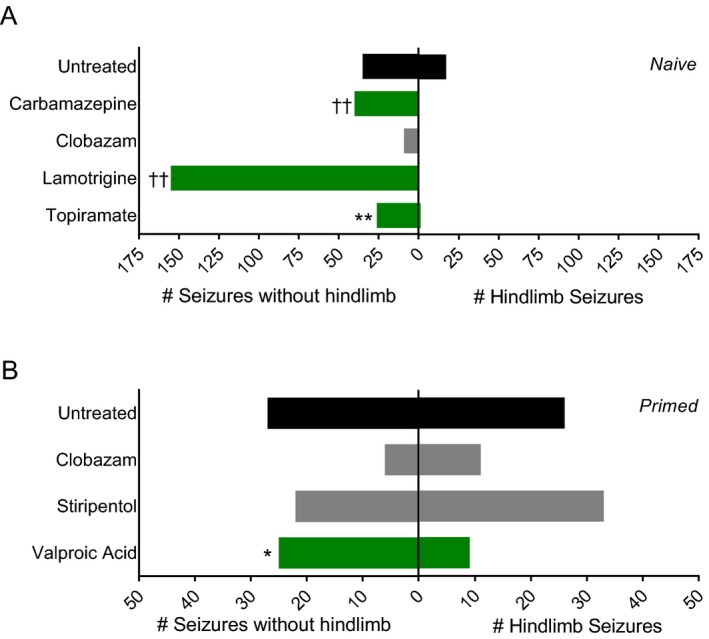
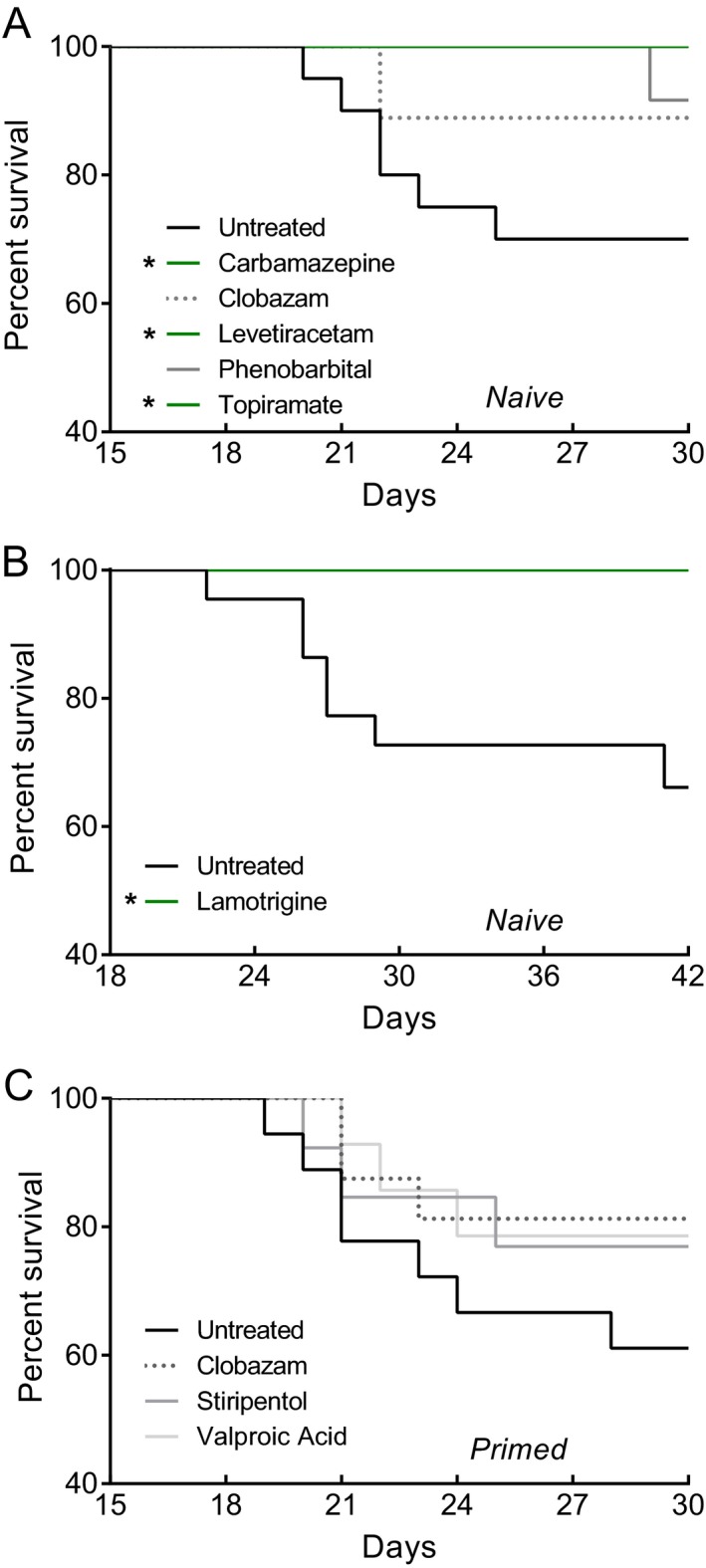
Results: Scn1a+/- mice exhibited responses to anticonvulsant treatment similar to those observed clinically. Sodium channel blockers were not effective or exacerbated seizures in Scn1a+/- mice. Overall, clobazam was the most effective anticonvulsant in Scn1a+/- mice, consistent with its effect in Dravet syndrome.
Interpretation: Genetic models of spontaneous epilepsy provide alternative screening platforms and may augment the AED development process. In this study, we established an effective screening platform that pharmacologically validated Scn1a+/- mice for preclinical screening of potential Dravet syndrome therapeutics.
Figures
References
-
- Golyala A, Kwan P. Drug development for refractory epilepsy: the past 25 years and beyond. Seizure 2017;44:147–156. - PubMed
-
- Dravet C, Oguni H. Chapter 65 ‐ Dravet syndrome (severe myoclonic epilepsy in infancy) In: Harvey BS, ed. Olivier Dulac ML. Handbook of Clinical Neurology: Elsevier, 2013:627–633. - PubMed
-
- Shmuely S, Sisodiya SM, Gunning WB, et al. Mortality in Dravet syndrome: a review. Epilepsy Behav 2016;64:Part A:69–Part A:74. - PubMed
-
- Shi X‐Y, Tomonoh Y, Wang W‐Z, et al. Efficacy of antiepileptic drugs for the treatment of Dravet syndrome with different genotypes. Brain Develop 2016;38:40–46. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
