

Clinical and bacteriological efficacy of twice daily topical retapamulin ointment 1% in the management of impetigo and other uncomplicated superficial skin infections
- PMID: 28491950
- PMCID: PMC5418665
- DOI: 10.1016/j.ijwd.2014.12.002
Clinical and bacteriological efficacy of twice daily topical retapamulin ointment 1% in the management of impetigo and other uncomplicated superficial skin infections
Abstract
Background: Cutaneous bacterial infections are common in children and adults and frequently are caused by Staphylococcus aureus (S. aureus). Treatment failures with topical agents are not uncommon and have been shown to be secondary to bacterial resistance.
Objective: To determine clinical and bacteriological efficacy of retapamulin ointment 1% in treatment of patients with cutaneous bacterial infections caused by methicillin-resistant S. aureus (MRSA) and other bacteria.
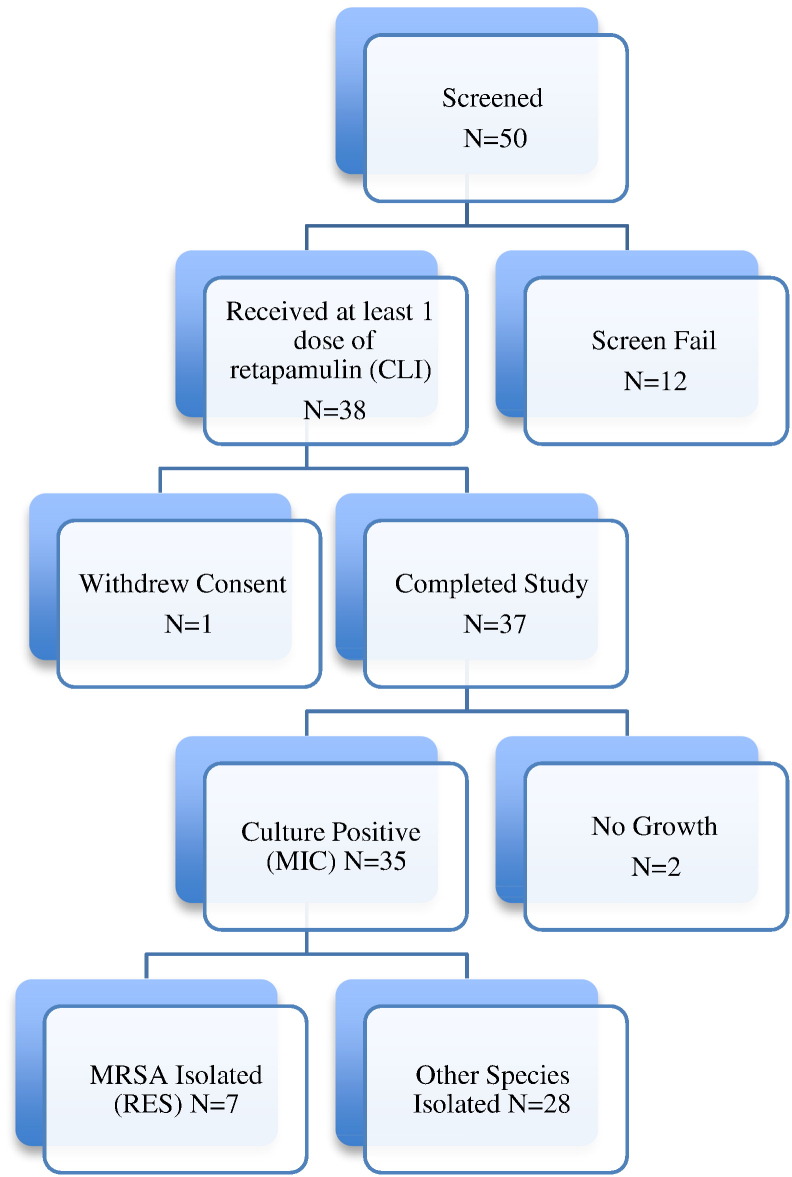
Methods: Prospective, nonrandomized, uncontrolled, open label, single center trial conducted between April 2008 and November 2012 that evaluated efficacy of retapamulin ointment 1% in the treatment of impetigo, folliculitis, and other minor soft tissue infections in children and adults. Fifty patients, who presented to a dermatology outpatient clinic and were clinically diagnosed with impetigo, folliculitis, or minor soft tissue infection suitable for treatment with a topical antibiotic, were screened. Thirty-eight patients were enrolled and received treatment: topical retapamulin ointment 1% twice daily for 5 days. Seven patients were MRSA positive and qualified for the primary efficacy population. One patient withdrew due to an adverse event. Clinical and microbiological exams were performed at baseline and follow-up 5 to 7 days later to assess clinical, microbiological, and therapeutic responses. Primary outcome was clinical response at follow-up in primary efficacy population with MRSA isolated as the baseline pathogen. Secondary outcomes included clinical, microbiologic, and therapeutic responses in patients who were culture positive for any species of bacteria.
Results: Clinical response at follow-up in the primary efficacy population (MRSA-positive patients) was not sufficiently powered to demonstrate significance; however, outcomes were excellent, with 7 of 7 patients demonstrating clinical success (5 of 7) or clinical improvement (2 of 7) at follow-up. Barring lack of significance due to small total sample size for patients who were culture positive for any species of bacteria (n = 35), overall success rates were favorable for clinical, microbiologic, and therapeutic responses with values of 66%, 97%, and 69%, respectively. Adverse events (AEs) were mild or moderate in severity. No serious AEs were reported.
Conclusion: Safety profile appears favorable given the low number of AEs. Study design limits conclusions that can be drawn. Nevertheless, this study supports use of topical retapamulin 1% ointment in treatment of cutaneous bacterial infections, particularly those caused by S. aureus, including MRSA.
Keywords: Impetigo; MRSA; MSSA; Pediatric; Retapamulin.
Figures
Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Topical antibiotics for preventing surgical site infection in wounds healing by primary intention.Cochrane Database Syst Rev. 2016 Nov 7;11(11):CD011426. doi: 10.1002/14651858.CD011426.pub2. Cochrane Database Syst Rev. 2016. PMID: 27819748 Free PMC article.
-
Antibiotics and antiseptics for venous leg ulcers.Cochrane Database Syst Rev. 2013 Dec 23;(12):CD003557. doi: 10.1002/14651858.CD003557.pub4. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2014 Jan 10;(1):CD003557. doi: 10.1002/14651858.CD003557.pub5. PMID: 24363048 Updated.
-
Interventions for Old World cutaneous leishmaniasis.Cochrane Database Syst Rev. 2017 Dec 1;12(12):CD005067. doi: 10.1002/14651858.CD005067.pub5. Cochrane Database Syst Rev. 2017. PMID: 29192424 Free PMC article.
-
Interventions for the eradication of meticillin-resistant Staphylococcus aureus (MRSA) in people with cystic fibrosis.Cochrane Database Syst Rev. 2022 Dec 13;12(12):CD009650. doi: 10.1002/14651858.CD009650.pub5. Cochrane Database Syst Rev. 2022. PMID: 36511181 Free PMC article.
Cited by
-
Intolerable Burden of Impetigo in Endemic Settings: A Review of the Current State of Play and Future Directions for Alternative Treatments.Antibiotics (Basel). 2020 Dec 15;9(12):909. doi: 10.3390/antibiotics9120909. Antibiotics (Basel). 2020. PMID: 33333955 Free PMC article. Review.
-
Impetigo Animal Models: A Review of Their Feasibility and Clinical Utility for Therapeutic Appraisal of Investigational Drug Candidates.Antibiotics (Basel). 2020 Oct 14;9(10):694. doi: 10.3390/antibiotics9100694. Antibiotics (Basel). 2020. PMID: 33066386 Free PMC article. Review.
-
Are Antimicrobial Peptide Dendrimers an Escape from ESKAPE?Adv Wound Care (New Rochelle). 2020 May 19;9(7):378-95. doi: 10.1089/wound.2019.1113. Online ahead of print. Adv Wound Care (New Rochelle). 2020. PMID: 32320368 Free PMC article.
-
New therapeutic applications of ozenoxacin in superficial skin infections.Dermatol Reports. 2021 Aug 5;14(2):9289. doi: 10.4081/dr.2021.9289. eCollection 2022 Jun 16. Dermatol Reports. 2021. PMID: 35795839 Free PMC article.
References
-
- Bangert S., Levy M., Hebert A.A. Bacterial resistance and impetigo treatment trends: a review. Pediatr Dermatol. 2012;29:243–248. - PubMed
-
- Bernard P. Management of common bacterial infections of the skin. Curr Opin Infect Dis. 2008;21:122–128. - PubMed
-
- Clinical and Laboratory Standards Institute . Seventeenth Informational Supplement. CLSI; Wayne, PA: 2007. Performance Standards for Antimicrobial Susceptibility Testing. (CLSI Document M100-S17)
-
- Cole C., Gazewood J. Diagnosis and treatment of impetigo. Am Fam Physician. 2007;75:859–864. - PubMed
-
- Darmstadt G.L., Lane A.T. Impetigo: an overview. Pediatr Dermatol. 1994;11:293–303. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
