

Association between a common immunoglobulin heavy chain allele and rheumatic heart disease risk in Oceania
- PMID: 28492228
- PMCID: PMC5437274
- DOI: 10.1038/ncomms14946
Association between a common immunoglobulin heavy chain allele and rheumatic heart disease risk in Oceania
Abstract
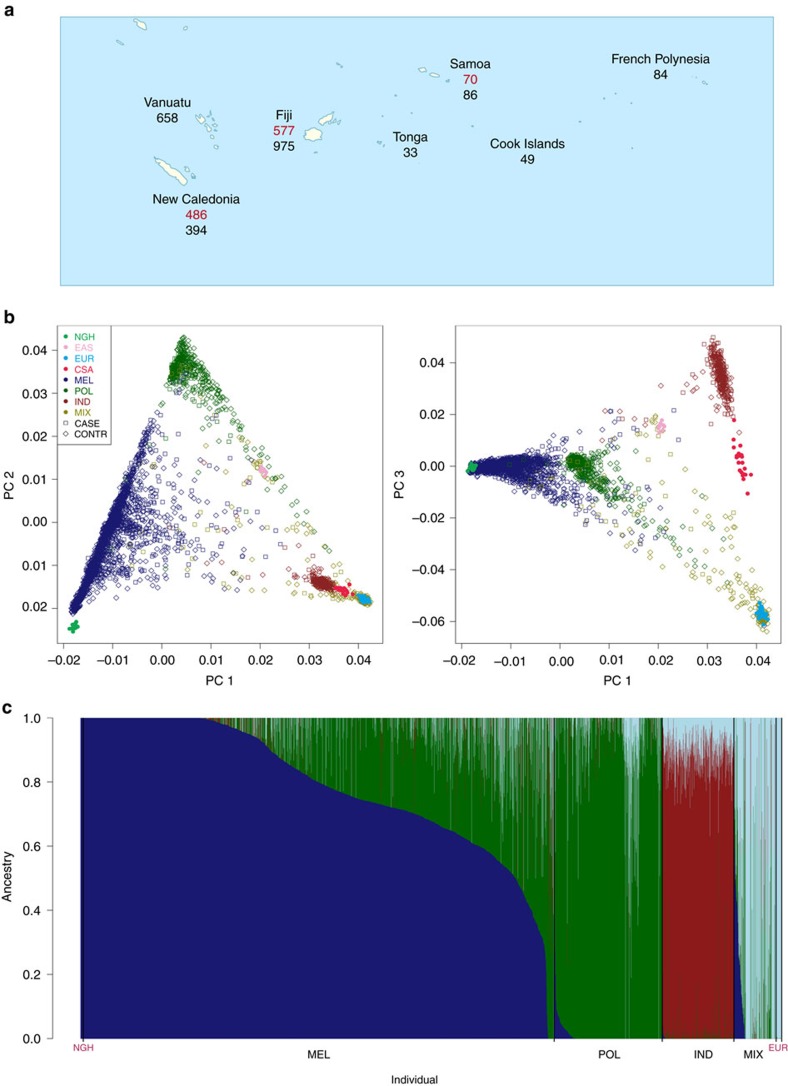
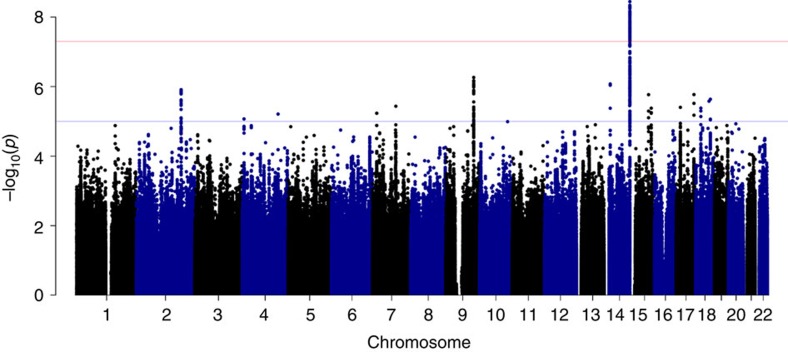
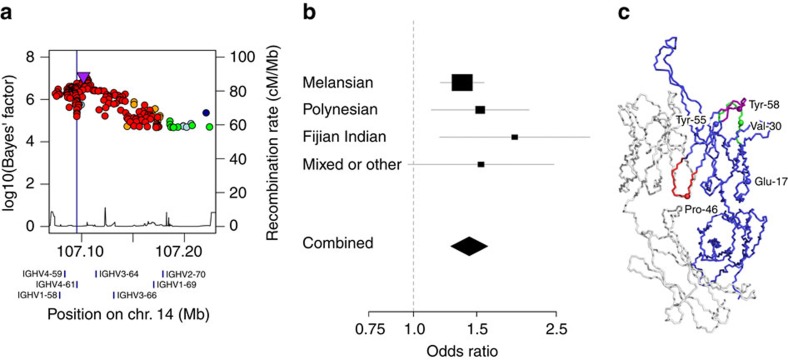
The indigenous populations of the South Pacific experience a high burden of rheumatic heart disease (RHD). Here we report a genome-wide association study (GWAS) of RHD susceptibility in 2,852 individuals recruited in eight Oceanian countries. Stratifying by ancestry, we analysed genotyped and imputed variants in Melanesians (607 cases and 1,229 controls) before follow-up of suggestive loci in three further ancestral groups: Polynesians, South Asians and Mixed or other populations (totalling 399 cases and 617 controls). We identify a novel susceptibility signal in the immunoglobulin heavy chain (IGH) locus centring on a haplotype of nonsynonymous variants in the IGHV4-61 gene segment corresponding to the IGHV4-61*02 allele. We show each copy of IGHV4-61*02 is associated with a 1.4-fold increase in the risk of RHD (odds ratio 1.43, 95% confidence intervals 1.27-1.61, P=4.1 × 10-9). These findings provide new insight into the role of germline variation in the IGH locus in disease susceptibility.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
References
-
- Steer A. C. & Carapetis J. R. Prevention and treatment of rheumatic heart disease in the developing world. Nat. Rev. Cardiol. 6, 689–698 (2009). - PubMed
-
- Carapetis J. R., Steer A. C., Mulholland E. K. & Weber M. The global burden of group A streptococcal diseases. Lancet Infect. Dis. 5, 685–694 (2005). - PubMed
-
- Reményi B. et al. Position statement of the World Heart Federation on the prevention and control of rheumatic heart disease. Nat. Rev. Cardiol. 10, 284–292 (2013). - PubMed
-
- Cheadle W. B. Barbeian Lectures on the various manifestations of the rheumatic state as exemplified in childhood and early life. Lancet 133, 821–827 (1889).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
