

Pediatric In-Hospital Acute Respiratory Compromise: A Report From the American Heart Association's Get With the Guidelines-Resuscitation Registry
- PMID: 28492403
- PMCID: PMC5581225
- DOI: 10.1097/PCC.0000000000001204
Pediatric In-Hospital Acute Respiratory Compromise: A Report From the American Heart Association's Get With the Guidelines-Resuscitation Registry
Abstract
Objectives: The main objectives of this study were to describe in-hospital acute respiratory compromise among children (< 18 yr old), and its association with cardiac arrest and in-hospital mortality.
Design: Observational study using prospectively collected data.
Setting: U.S. hospitals reporting data to the "Get With The Guidelines-Resuscitation" registry.
Patients: Pediatric patients (< 18 yr old) with acute respiratory compromise. Acute respiratory compromise was defined as absent, agonal, or inadequate respiration that required emergency assisted ventilation and elicited a hospital-wide or unit-based emergency response.
Interventions: None.
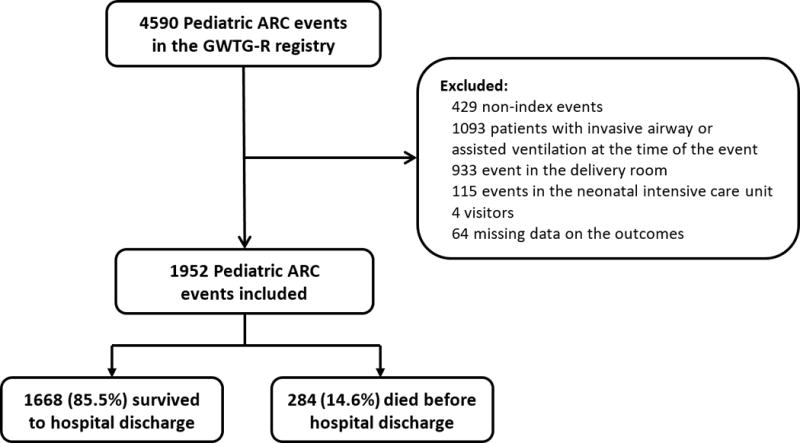
Measurements and main results: The primary outcome was in-hospital mortality. Cardiac arrest during the event was a secondary outcome. To assess the association between patient, event, and hospital characteristics and the outcomes, we created multivariable logistic regressions models accounting for within-hospital clustering. One thousand nine hundred fifty-two patients from 151 hospitals were included. Forty percent of the events occurred on the wards, 19% in the emergency department, 25% in the ICU, and 16% in other locations. Two hundred eighty patients (14.6%) died before hospital discharge. Preexisting hypotension (odds ratio, 3.26 [95% CI, 1.89-5.62]; p < 0.001) and septicemia (odds ratio, 2.46 [95% CI, 1.52-3.97]; p < 0.001) were associated with increased mortality. The acute respiratory compromise event was temporally associated with a cardiac arrest in 182 patients (9.3%), among whom 46.2% died. One thousand two hundred eight patients (62%) required tracheal intubation during the event. In-hospital mortality among patients requiring tracheal intubation during the event was 18.6%.
Conclusions: In this large, multicenter study of acute respiratory compromise, 40% occurred in ward settings, 9.3% had an associated cardiac arrest, and overall in-hospital mortality was 14.6%. Preevent hypotension and septicemia were associated with increased mortality rate.
Conflict of interest statement
The authors have no conflicts of interest relevant to this article to disclose.
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Acute Respiratory Compromise Leading to Cardiac Arrest.Pediatr Crit Care Med. 2017 Sep;18(9):894-895. doi: 10.1097/PCC.0000000000001233. Pediatr Crit Care Med. 2017. PMID: 28863090 No abstract available.
References
-
- Randolph AG, Meert KL, O’Neil ME, et al. The feasibility of conducting clinical trials in infants and children with acute respiratory failure. Am J Respir Crit Care Med. 2003;167(10):1334–1340. - PubMed
-
- Leclerc F, Duhamel A, Deken V, et al. Nonrespiratory pediatric logistic organ dysfunction-2 score is a good predictor of mortality in children with acute respiratory failure. Pediatr Crit Care Med. 2014;15(7):590–593. - PubMed
-
- Rivera RA, Butt W, Shann F. Predictors of mortality in children with respiratory failure: possible indications for ECMO. Anaesth Intensive Care. 1990;18(3):385–389. - PubMed
-
- Timmons OD, Havens PL, Fackler JC. Predicting death in pediatric patients with acute respiratory failure. Pediatric Critical Care Study Group. Extracorporeal Life Support Organization. Chest. 1995;108(3):789–797. - PubMed
-
- Behrendt CE. Acute respiratory failure in the United States: incidence and 31-day survival. Chest. 2000;118(4):1100–1105. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
