

Enhanced Recovery After Surgery Program Implementation in 2 Surgical Populations in an Integrated Health Care Delivery System
- PMID: 28492816
- PMCID: PMC5568841
- DOI: 10.1001/jamasurg.2017.1032
Enhanced Recovery After Surgery Program Implementation in 2 Surgical Populations in an Integrated Health Care Delivery System
Abstract
Importance: Novel approaches to perioperative surgical care focus on optimizing nutrition, mobility, and pain management to minimize adverse events after surgical procedures.
Objective: To evaluate the outcomes of an enhanced recovery after surgery (ERAS) program among 2 target populations: patients undergoing elective colorectal resection and patients undergoing emergency hip fracture repair.
Design, setting, and participants: A pre-post difference-in-differences study before and after ERAS implementation in the target populations compared with contemporaneous surgical comparator groups (patients undergoing elective gastrointestinal surgery and emergency orthopedic surgery). Implementation began in February and March 2014 and concluded by the end of 2014 at 20 medical centers within the Kaiser Permanente Northern California integrated health care delivery system.
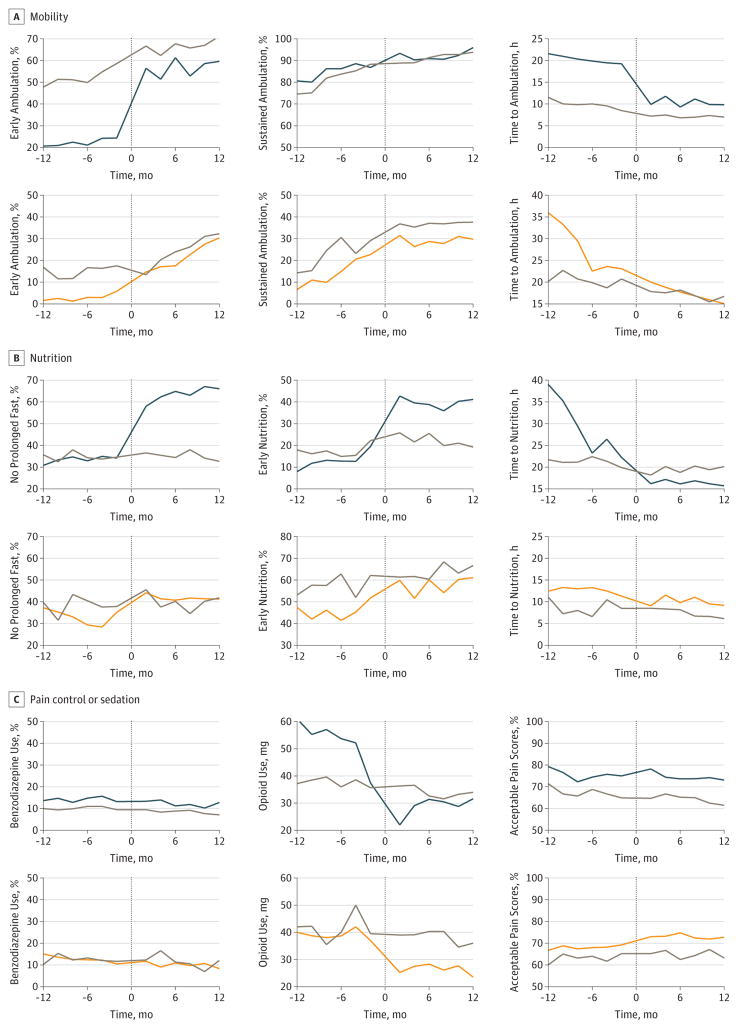
Exposures: A multifaceted ERAS program designed with a particular focus on perioperative pain management, mobility, nutrition, and patient engagement.
Main outcomes and measures: The primary outcome was hospital length of stay. Secondary outcomes included hospital mortality, home discharge, 30-day readmission rates, and complication rates.
Results: The study included a total of 3768 patients undergoing elective colorectal resection (mean [SD] age, 62.7 [14.1] years; 1812 [48.1%] male) and 5002 patients undergoing emergency hip fracture repair (mean [SD] age, 79.5 [11.8] years; 1586 [31.7%] male). Comparator surgical patients included 5556 patients undergoing elective gastrointestinal surgery and 1523 patients undergoing emergency orthopedic surgery. Most process metrics had significantly greater changes in the ERAS target populations after implementation compared with comparator surgical populations, including those for ambulation, nutrition, and opioid use. Hospital length of stay and postoperative complication rates were also significantly lower among ERAS target populations after implementation. The rate ratios for postoperative complications were 0.68 (95% CI, 0.46-0.99; P = .04) for patients undergoing colorectal resection and 0.67 (95% CI, 0.45-0.99, P = .05) for patients with hip fracture. Among patients undergoing colorectal resection, ERAS implementation was associated with decreased rates of hospital mortality (0.17; 95% CI, 0.03-0.86; P = .03), whereas among patients with hip fracture, implementation was associated with increased rates of home discharge (1.24; 95% CI, 1.06-1.44; P = .007).
Conclusions and relevance: Multicenter implementation of an ERAS program among patients undergoing elective colorectal resection and patients undergoing emergency hip fracture repair successfully altered processes of care and was associated with significant absolute and relative decreases in hospital length of stay and postoperative complication rates. Rapid, large-scale implementation of a multidisciplinary ERAS program is feasible and effective in improving surgical outcomes.
Conflict of interest statement
Figures
Comment in
-
Enhanced Surgical Recovery Through Enhanced Research From Integrated Health Systems.JAMA Surg. 2017 Jul 19;152(7):e171051. doi: 10.1001/jamasurg.2017.1051. Epub 2017 Jul 19. JAMA Surg. 2017. PMID: 28492815 No abstract available.
References
-
- Kohn LT, Corrigan JM, Donaldson MS. To Err Is Human: Building a Safer Health System. Washington, DC: National Academies Press; 1999. - PubMed
-
- Number of all-listed procedures for discharges from short-stay hospitals, by procedure category and age: United States, 2010. Centers for Disease Control and Prevention; [Accessed October 5, 2016]. http://www.cdc.gov/nchs/data/nhds/4procedures/2010pro4_numberprocedureag....
-
- Vonlanthen R, Slankamenac K, Breitenstein S, et al. The impact of complications on costs of major surgical procedures: a cost analysis of 1200 patients. Ann Surg. 2011;254(6):907–913. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
