

The Epidemiology of Emergency Department Trauma Discharges in the United States
- PMID: 28493608
- PMCID: PMC5647215
- DOI: 10.1111/acem.13223
The Epidemiology of Emergency Department Trauma Discharges in the United States
Abstract
Objective: Injury-related morbidity and mortality is an important emergency medicine and public health challenge in the United States. Here we describe the epidemiology of traumatic injury presenting to U.S. emergency departments (EDs), define changes in types and causes of injury among the elderly and the young, characterize the role of trauma centers and teaching hospitals in providing emergency trauma care, and estimate the overall economic burden of treating such injuries.
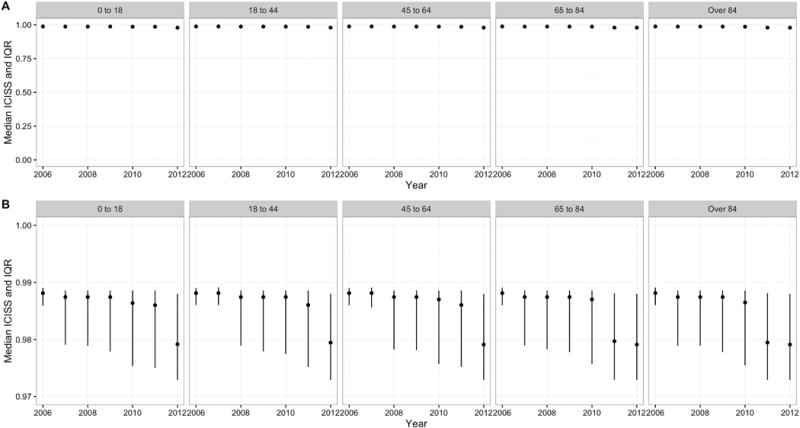
Methods: We conducted a secondary retrospective, repeated cross-sectional study of the Nationwide Emergency Department Data Sample (NEDS), the largest all-payer ED survey database in the United States. Main outcomes and measures were survey-adjusted counts, proportions, means, and rates with associated standard errors (SEs) and 95% confidence intervals. We plotted annual age-stratified ED discharge rates for traumatic injury and present tables of proportions of common injuries and external causes. We modeled the association of Level I or II trauma center care with injury fatality using a multivariable survey-adjusted logistic regression analysis that controlled for age, sex, injury severity, comorbid diagnoses, and teaching hospital status.
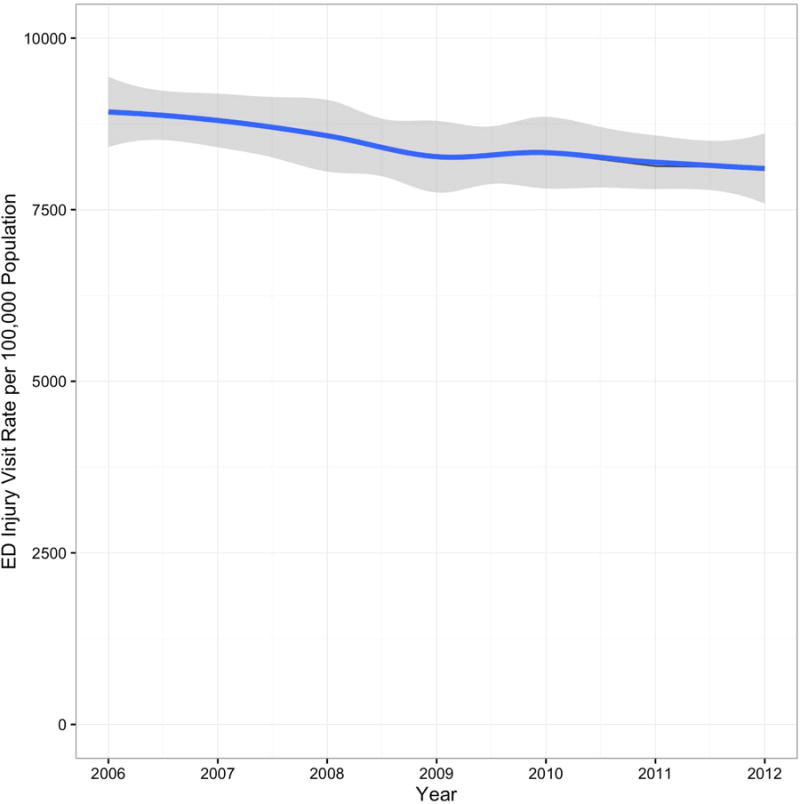
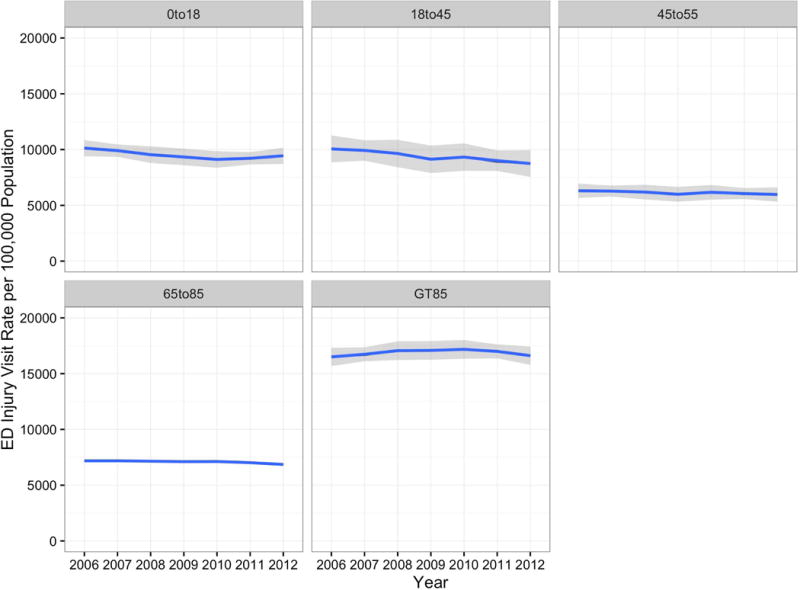
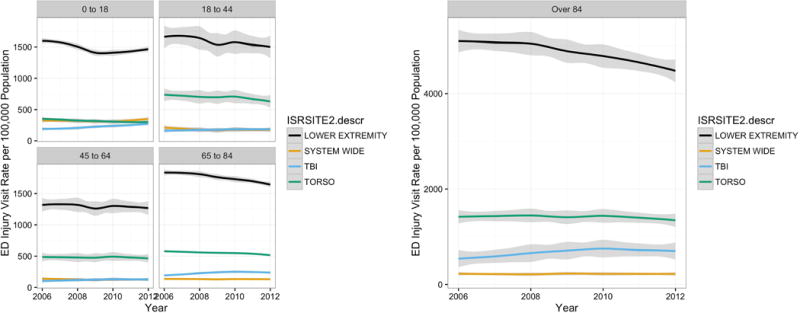
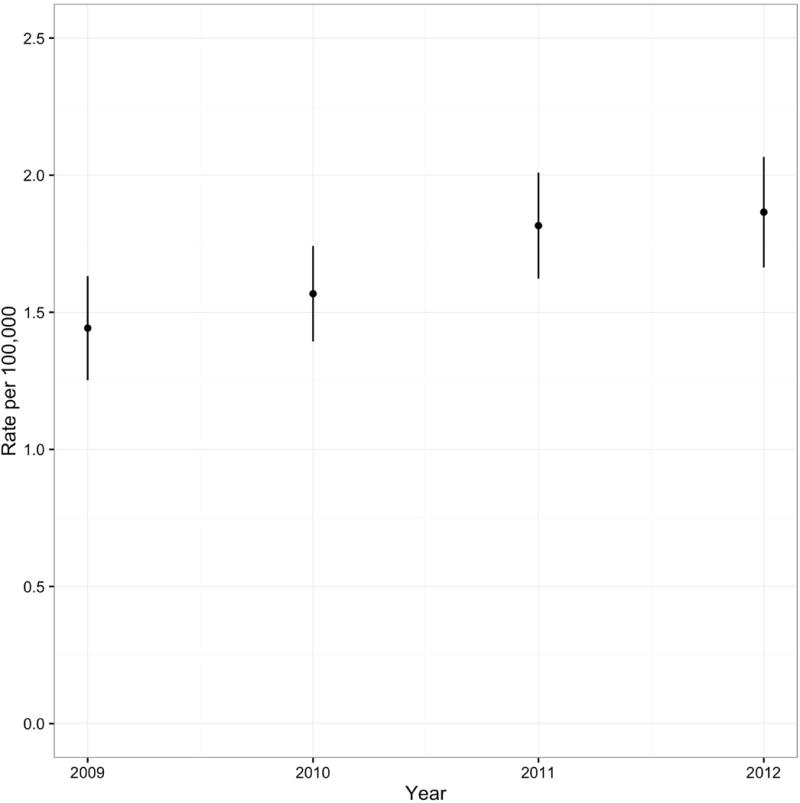
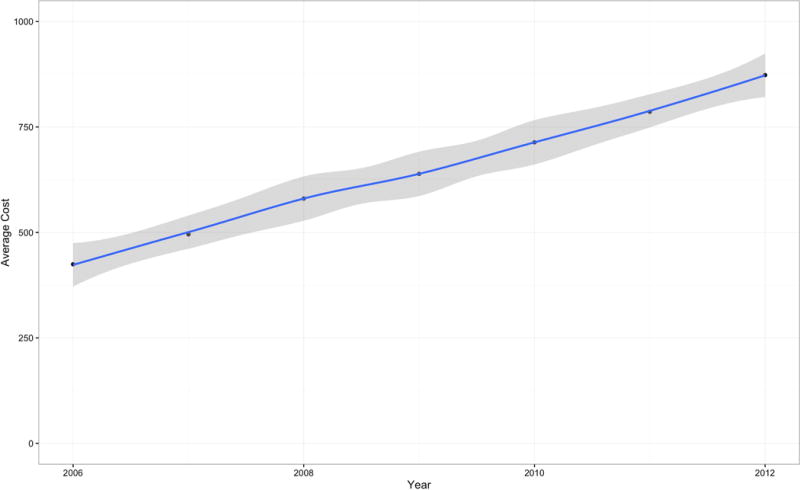
Results: There were 181,194,431 (SE = 4,234) traumatic injury discharges from U.S. EDs between 2006 and 2012. There was a mean year-to-year decrease of 143 (95% CI = -184.3 to -68.5) visits per 100,000 U.S. population during the study period. The all-age, all-cause case-fatality rate for traumatic injuries across U.S. EDs during the study period was 0.17% (SE = 0.001%). The case-fatality rate for the most severely injured averaged 4.8% (SE = 0.001%), and severely injured patients were nearly four times as likely to be seen in Level I or II trauma centers (relative risk = 3.9 [95% CI = 3.7 to 4.1]). The unadjusted risk ratio, based on group counts, for the association of Level I or II trauma centers with mortality was risk ratio = 4.9 (95% CI = 4.5 to 5.3); however, after sex, age, injury severity, and comorbidities were accounted for, Level I or II trauma centers were not associated with an increased risk of fatality (odds ratio = 0.96 [95% CI = 0.79 to 1.18]). There were notable changes at the extremes of age in types and causes of ED discharges for traumatic injury between 2009 and 2012. Age-stratified rates of diagnoses of traumatic brain injury increased 29.5% (SE = 2.6%) for adults older than 85 and increased 44.9% (SE = 1.3%) for children younger than 18. Firearm-related injuries increased 31.7% (SE = 0.2%) in children 5 years and younger. The total inflation-adjusted cost of ED injury care in the United States between 2006 and 2012 was $99.75 billion (SE = $0.03 billion).
Conclusions: Emergency departments are a sensitive barometer of the continuing impact of traumatic injury as an important cause of morbidity and mortality in the United States. Level I or II trauma centers remain a bulwark against the tide of severe trauma in the United States, but the types and causes of traumatic injury in the United States are changing in consequential ways, particularly at the extremes of age, with traumatic brain injuries and firearm-related trauma presenting increased challenges.
© 2017 by the Society for Academic Emergency Medicine.
Conflict of interest statement
Figures
References
-
- Web-based injury statistics query and reporting system (WISQARS), Leading causes of death reports, national and regional, 1999-2014. Centers for Disease Control and Prevention; [Accessed Sept 11, 2016]. http://webappa.cdc.gov/sasweb/ncipc/leadcaus10_us.html. Published June 24, 2015.
-
- Segui-Gomez M, MacKenzie E. Measuring the public health impact of injuries. Epidemiol Rev. 2003;25:3–19. - PubMed
-
- Web-based injury statistics query and reporting system (WISQARS), Leading causes of nonfatal injury reports, 2001-2014. Centers for Disease Control and Prevention; [Accessed Sept 10, 2016]. http://webappa.cdc.gov/sasweb/ncipc/nfilead2001.html Published March 28, 2013.
-
- Web-based injury statistics query and reporting system (WISQARS), Cost of injuries and violence in the United States. Centers for Disease Control and Prevention; [Accessed Sept 11, 2016]. http://www.cdc.gov/injury/wisqars/overview/cost_of_injury.html Published July 29, 2016.
-
- Bonnie RJ, Fulco CE, Liverman CT, editors. Reducing the burden of injury: advancing prevention and treatment. Washington, D.C.: National Academies Press; 1999. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
