

Melioidosis: Clinical impact and public health threat in the tropics
- PMID: 28493905
- PMCID: PMC5426594
- DOI: 10.1371/journal.pntd.0004738
Melioidosis: Clinical impact and public health threat in the tropics
Retraction in
-
Retraction: Melioidosis: Clinical impact and public health threat in the tropics.PLoS Negl Trop Dis. 2020 Jul 1;14(7):e0008441. doi: 10.1371/journal.pntd.0008441. eCollection 2020 Jul. PLoS Negl Trop Dis. 2020. PMID: 32609720 Free PMC article. No abstract available.
Abstract
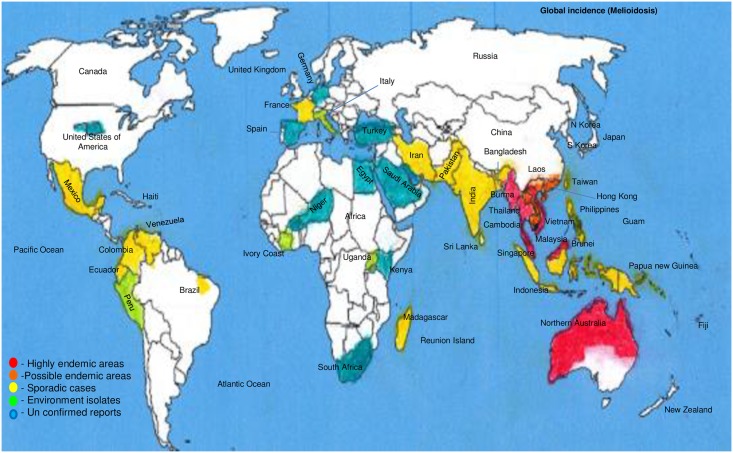
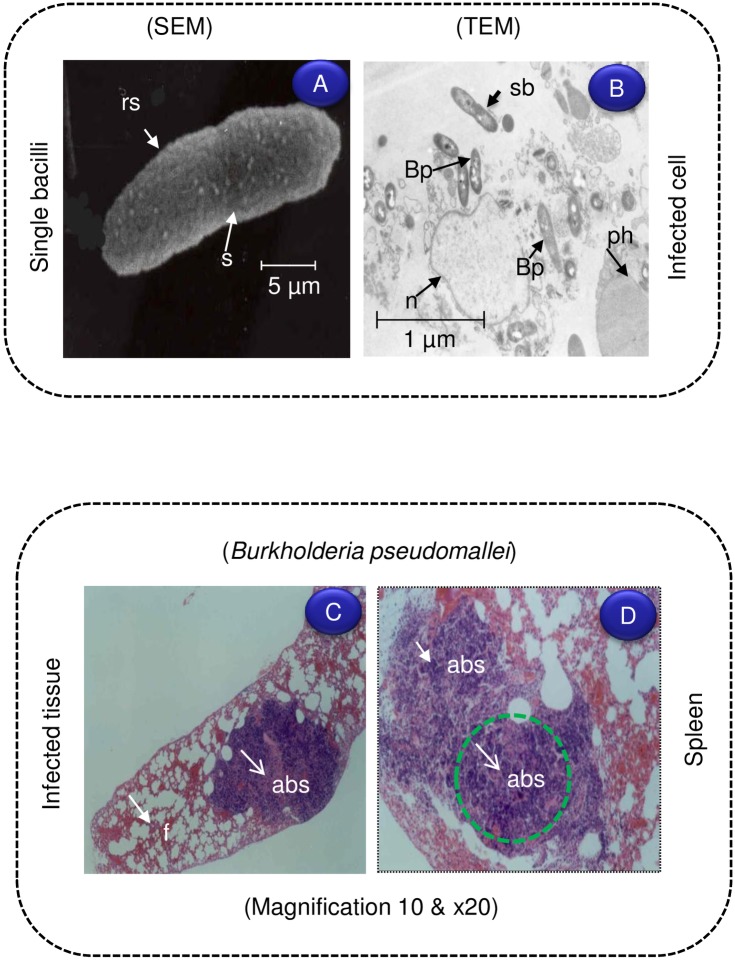
This review briefly summarizes the geographical distribution and clinical impact of melioidosis, especially in the tropics. Burkholderia pseudomallei (a gram-negative bacterium) is the major causative agent for melioidosis, which is prevalent in Singapore, Malaysia, Thailand, Vietnam, and Northern Australia. Melioidosis patients are increasingly being recognized in other parts of the world. The bacteria are intrinsically resistant to many antimicrobial agents, but prolonged treatment, especially with combinations of antibiotics, may be effective. Despite therapy, the overall case fatality rate of septicemia in melioidosis remains significantly high. Intracellular survival of the bacteria within macrophages may progress to chronic infections, and about 10% of patients suffer relapses. In the coming decades, melioidosis will increasingly afflict travelers throughout many global regions. Clinicians managing travelers returning from the subtropics or tropics with severe pneumonia or septicemia should consider acute melioidosis as a differential diagnosis. Patients with open skin wounds, diabetes, or chronic renal disease are at higher risk for melioidosis and should avoid direct contact with soil and standing water in endemic regions. Furthermore, there are fears that B. pseudomallei may be used as a biological weapon. Technological advancements in molecular diagnostics and antibiotic therapy are improving the disease outcomes in endemic areas throughout Asia. Research and development efforts on vaccine candidates against melioidosis are ongoing.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


Comment in
-
Melioidosis: The hazards of incomplete peer-review.PLoS Negl Trop Dis. 2019 Mar 14;13(3):e0007123. doi: 10.1371/journal.pntd.0007123. eCollection 2019 Mar. PLoS Negl Trop Dis. 2019. PMID: 30870410 Free PMC article. No abstract available.
References
-
- Krishnaswami CS (1917) Morphia injectors septicaemia. Indian Med Gazette 52: 296–299.
-
- Stanton AT, Fletcher W (1921) Melioidosis, a new disease of the tropics Far Eastern Association of Tropical Medicine: Transactions of the Fourth Congress. Batavia, Dutch East Indies: (Javasche Boekhandel en Drukkerij; ).
-
- Short BH (2002). Melioidosis: an important emerging infectious disease-a military problem?. ADF Health 3: 13–21.
-
- Thomas AD, Forbes Faulkner J, Parker M (1979) Isolation of P. pseudomallei from clay layers at different depths. Am J Epidemiol 110: 515–521. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
