

Prediction of pancreatic fistula after pancreatoduodenectomy by preoperative dynamic CT and fecal elastase-1 levels
- PMID: 28493949
- PMCID: PMC5426704
- DOI: 10.1371/journal.pone.0177052
Prediction of pancreatic fistula after pancreatoduodenectomy by preoperative dynamic CT and fecal elastase-1 levels
Abstract
Objective: To validate preoperative dynamic CT and fecal elastase-1 level in predicting the development of pancreatic fistulae after pancreatoduodenectomy.
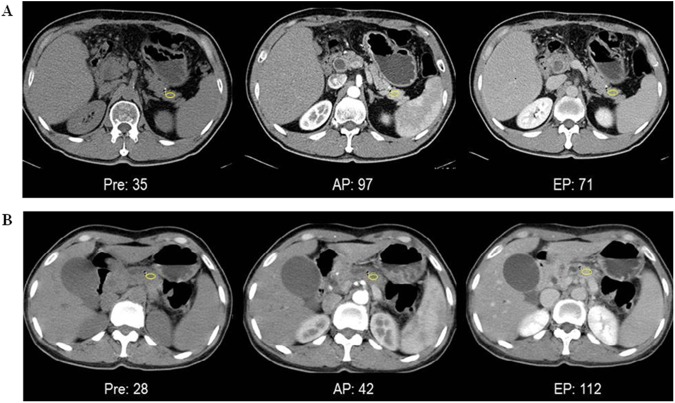
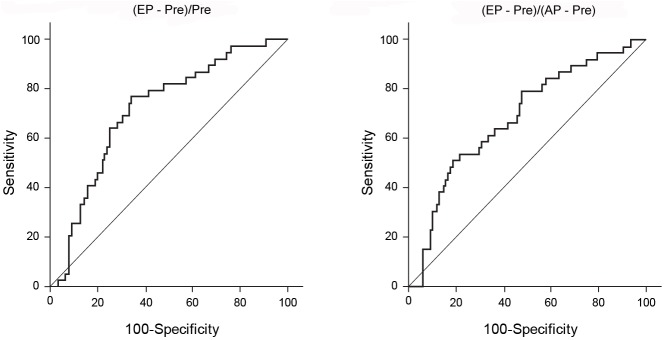
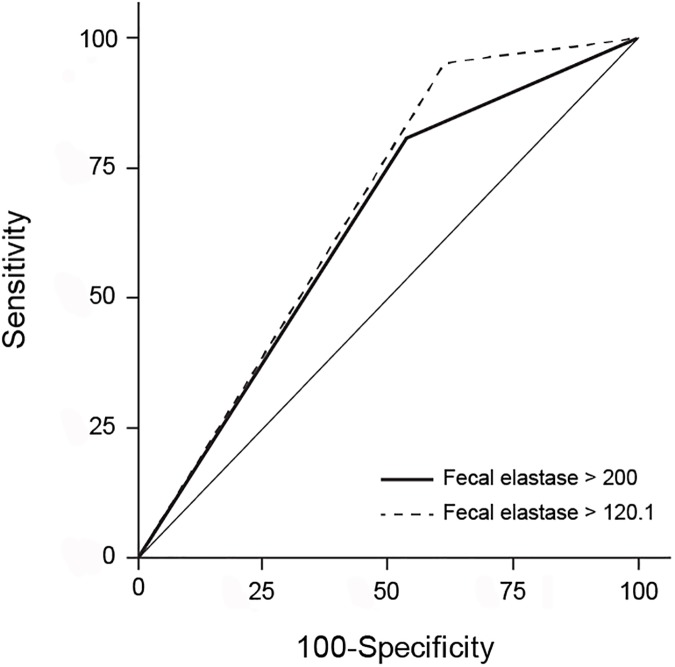
Materials and methods: For 146 consecutive patients, CT attenuation values of the nontumorous pancreatic parenchyma were retrospectively measured on precontrast, arterial and equilibrium phase images for calculation of enhancement ratios. CT enhancement ratios and preoperative fecal elastase-1 levels were correlated with the development of pancreatic fistulae using independent t-test, logistic regression models, ROC analysis, Youden method and tree analysis.
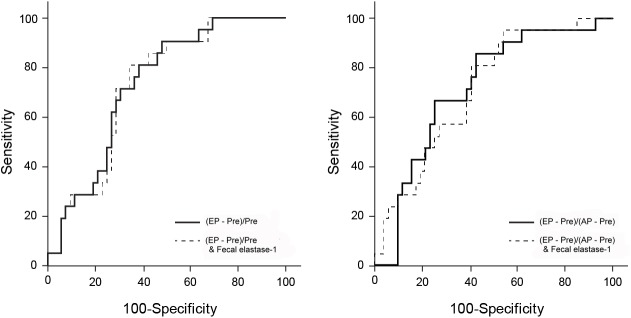
Results: The mean value of enhancement ratio on equilibrium phase was significantly higher (p = 0.001) in the patients without pancreatic fistula (n = 107; 2.26±3.63) than in the patients with pancreatic fistula (n = 39; 1.04±0.51); in the logistic regression analyses, it was significant predictor for the development of pancreatic fistulae (odds ratio = 0.243, p = 0.002). The mean preoperative fecal elastase-1 levels were higher (odds ratio = 1.003, p = 0.034) in the pancreatic fistula patients than other patients, but there were no significant differences in the areas under the curve between the prediction values of CT enhancement ratios and fecal elastase-1 combined and those of CT enhancement ratios alone (P = 0.897, p = 0.917) on ROC curve analysis. Tree analysis revealed that the CT enhancement ratio was more powerful predictor of pancreatic fistula than fecal elastase-1 levels.
Conclusion: The preoperative CT enhancement ratio of pancreas acquired at equilibrium phase regardless of combination with fecal elastase-1 levels might be a useful predictor of the risk of developing a pancreatic fistula following pancreatoduodenectomy.
Conflict of interest statement
Figures


Similar articles
-
[Clinical study on the relationship between pancreatic fistula and the degree of pancreatic fibrosis after pancreatic and duodenal resection].Zhonghua Wai Ke Za Zhi. 2017 May 1;55(5):373-377. doi: 10.3760/cma.j.issn.0529-5815.2017.05.013. Zhonghua Wai Ke Za Zhi. 2017. PMID: 28464579 Chinese.
-
The attenuation value of preoperative computed tomography as a novel predictor for pancreatic fistula after pancreaticoduodenectomy.Surg Today. 2018 Jun;48(6):598-608. doi: 10.1007/s00595-018-1626-y. Epub 2018 Jan 30. Surg Today. 2018. PMID: 29383597
-
Computed Tomography Enhancement Pattern of the Pancreatic Parenchyma Predicts Postoperative Pancreatic Fistula After Pancreaticoduodenectomy.Pancreas. 2019 Feb;48(2):209-215. doi: 10.1097/MPA.0000000000001229. Pancreas. 2019. PMID: 30589830
-
Preoperative imaging evaluation of pancreatic pathologies for the objective prediction of pancreatic fistula after pancreaticoduodenectomy.Surg Today. 2018 Feb;48(2):140-150. doi: 10.1007/s00595-017-1529-3. Epub 2017 Apr 18. Surg Today. 2018. PMID: 28421350 Review.
-
Predicting post-operative pancreatic fistulae using preoperative pancreatic imaging: a systematic review.ANZ J Surg. 2019 Jun;89(6):659-665. doi: 10.1111/ans.14891. Epub 2018 Oct 10. ANZ J Surg. 2019. PMID: 30306712
Cited by
-
Preoperative CT texture features predict prognosis after curative resection in pancreatic cancer.Sci Rep. 2019 Nov 22;9(1):17389. doi: 10.1038/s41598-019-53831-w. Sci Rep. 2019. PMID: 31757989 Free PMC article.
-
The usefulness of preoperative exocrine function evaluated by the 13C-trioctanoin breath test as a significant physiological predictor of pancreatic fistula after pancreaticoduodenectomy.BMC Surg. 2022 Feb 11;22(1):49. doi: 10.1186/s12893-022-01500-7. BMC Surg. 2022. PMID: 35148748 Free PMC article.
-
Do preoperative pancreatic computed tomography attenuation index and enhancement ratio predict pancreatic fistula after pancreaticoduodenectomy?World J Radiol. 2022 Jun 28;14(6):165-176. doi: 10.4329/wjr.v14.i6.165. World J Radiol. 2022. PMID: 35978980 Free PMC article.
-
Postoperative pancreatic fistula: a review of traditional and emerging concepts.Clin Exp Gastroenterol. 2018 Mar 15;11:105-118. doi: 10.2147/CEG.S120217. eCollection 2018. Clin Exp Gastroenterol. 2018. PMID: 29588609 Free PMC article. Review.
-
Radiological parameters to predict pancreatic texture: Current evidence and future perspectives.World J Radiol. 2023 Jun 28;15(6):170-181. doi: 10.4329/wjr.v15.i6.170. World J Radiol. 2023. PMID: 37424737 Free PMC article. Review.
References
-
- Richter A, Niedergethmann M, Sturm JW, Lorenz D, Post S, Trede M. Long-term results of partial pancreaticoduodenectomy for ductal adenocarcinoma of the pancreatic head: 25-year experience. World J Surg 2003;27:324–9. doi: 10.1007/s00268-002-6659-z - DOI - PubMed
-
- Adam U, Makowiec F, Riediger H, Schareck WD, Benz S, Hopt UT. Risk factors for complications after pancreatic head resection. Am J Surg 2004;187:201–8. doi: 10.1016/j.amjsurg.2003.11.004 - DOI - PubMed
-
- DeOliveira ML, Winter JM, Schafer M, Cunningham SC, Cameron JL, Yeo CJ, et al. Assessment of complications after pancreatic surgery: A novel grading system applied to 633 patients undergoing pancreaticoduodenectomy. Ann Surg 2006;244:931–7; discussion 7–9. doi: 10.1097/01.sla.0000246856.03918.9a - DOI - PMC - PubMed
-
- Hashimoto Y, Traverso LW. Incidence of pancreatic anastomotic failure and delayed gastric emptying after pancreatoduodenectomy in 507 consecutive patients: Use of a web-based calculator to improve homogeneity of definition. Surgery 2010;147:503–15. doi: 10.1016/j.surg.2009.10.034 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
