

Efficacy and Adverse Effects of Atropine in Childhood Myopia: A Meta-analysis
- PMID: 28494063
- PMCID: PMC5710262
- DOI: 10.1001/jamaophthalmol.2017.1091
Efficacy and Adverse Effects of Atropine in Childhood Myopia: A Meta-analysis
Abstract
Importance: Some uncertainty about the clinical value and dosing of atropine for the treatment of myopia in children remains.
Objective: To evaluate the efficacy vs the adverse effects of various doses of atropine in the therapy for myopia in children.
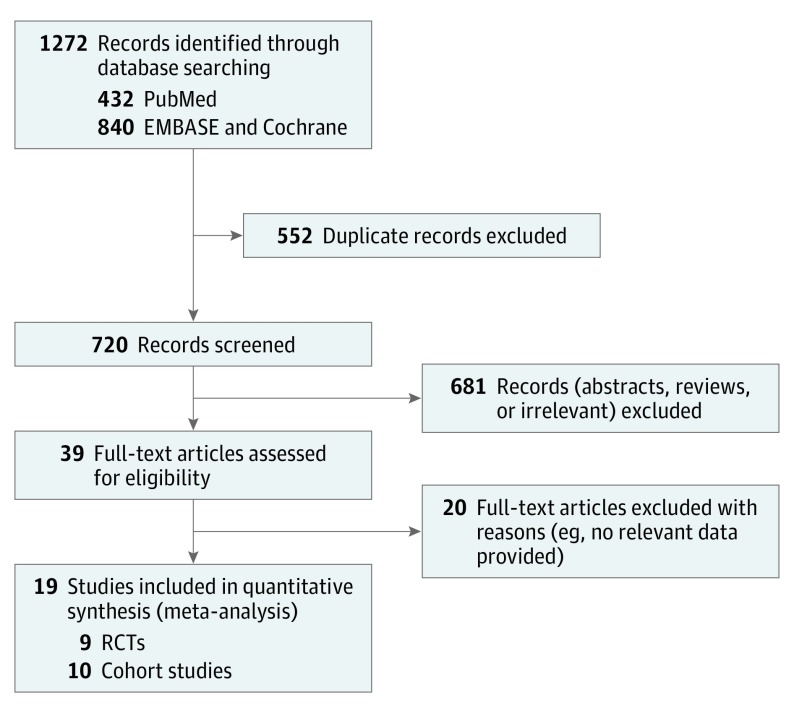
Data sources: Data were obtained from PubMed, EMBASE, and the Cochrane Central Register of Controlled Trials, from inception to April 30, 2016. The reference lists of published reviews and clinicaltrials.gov were searched for additional relevant studies. Key search terms included myopia, refractive errors, and atropine. Only studies published in English were included.
Study selection: Randomized clinical trials and cohort studies that enrolled patients younger than 18 years with myopia who received atropine in at least 1 treatment arm and that reported the annual rate of myopia progression and/or any adverse effects of atropine therapy were included in the analysis.
Data extraction and synthesis: Two reviewers independently abstracted the data. Heterogeneity was statistically quantified by Q, H, and I2 statistics, and a meta-analysis was performed using the random-effects model. The Cochrane Collaboration 6 aspects of bias and the Newcastle-Ottawa Scale were used to assess the risk for bias.
Main outcomes and measures: The primary outcome was a difference in efficacy and the presence of adverse effects at different doses of atropine vs control conditions. The secondary outcomes included the differences in adverse effects between Asian and white patients.
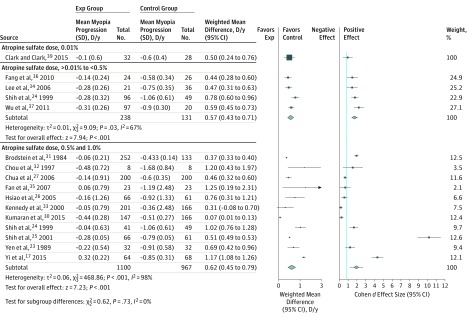
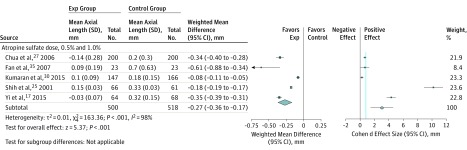
Results: Nineteen unique studies involving 3137 unique children were included in the analysis. The weighted mean differences between the atropine and control groups in myopia progression were 0.50 diopters (D) per year (95% CI, 0.24-0.76 D per year) for low-dose atropine, 0.57 D per year (95% CI, 0.43-0.71 D per year) for moderate-dose atropine, and 0.62 D per year (95% CI, 0.45-0.79 D per year) for high-dose atropine (P < .001), which translated to a high effect size (Cohen d, 0.97, 1.76, and 1.94, respectively). All doses of atropine, therefore, were equally beneficial with respect to myopia progression (P = .15). High-dose atropine were associated with more adverse effects, such as the 43.1% incidence of photophobia compared with 6.3% for low-dose atropine and 17.8% for moderate-dose atropine (χ22 = 7.05; P = .03). In addition, differences in the incidence of adverse effects between Asian and white patients were not identified (χ21 = 0.81; P = .37 for photophobia).
Conclusions and relevance: This meta-analysis suggests that the efficacy of atropine is dose independent within this range, whereas the adverse effects are dose dependent.
Conflict of interest statement
Figures
Comment in
-
Low-Dose Atropine for Myopia Control: Considering All the Data.JAMA Ophthalmol. 2018 Mar 1;136(3):303. doi: 10.1001/jamaophthalmol.2017.6638. JAMA Ophthalmol. 2018. PMID: 29423500 No abstract available.
-
Low-Dose Atropine for Myopia Control-Reply.JAMA Ophthalmol. 2018 Mar 1;136(3):303-304. doi: 10.1001/jamaophthalmol.2017.6641. JAMA Ophthalmol. 2018. PMID: 29423510 No abstract available.
References
-
- Dolgin E. The myopia boom. Nature. 2015;519(7543):276-278. - PubMed
-
- Morgan IG, Ohno-Matsui K, Saw SM. Myopia. Lancet. 2012;379(9827):1739-1748. - PubMed
-
- Fan DS, Lam DS, Lam RF, et al. Prevalence, incidence, and progression of myopia of school children in Hong Kong. Invest Ophthalmol Vis Sci. 2004;45(4):1071-1075. - PubMed
-
- Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singapore. 2004;33(1):27-33. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
