

Neurologic Serious Adverse Events Associated with Nivolumab Plus Ipilimumab or Nivolumab Alone in Advanced Melanoma, Including a Case Series of Encephalitis
- PMID: 28495807
- PMCID: PMC5469590
- DOI: 10.1634/theoncologist.2016-0487
Neurologic Serious Adverse Events Associated with Nivolumab Plus Ipilimumab or Nivolumab Alone in Advanced Melanoma, Including a Case Series of Encephalitis
Abstract
Background: Despite unprecedented efficacy across multiple tumor types, immune checkpoint inhibitor therapy is associated with a unique and wide spectrum of immune-related adverse events (irAEs), including neurologic events ranging from mild headache to potentially life-threatening encephalitis. Here, we summarize neurologic irAEs associated with nivolumab and ipilimumab melanoma treatment, present cases of treatment-related encephalitis, and provide practical guidance on diagnosis and management.
Methods: We searched a Global Pharmacovigilance and Epidemiology database for neurologic irAEs reported over an 8-year period in patients with advanced melanoma receiving nivolumab with or without ipilimumab from 12 studies sponsored by Bristol-Myers Squibb. Serious neurologic irAEs were reviewed, and relationship to nivolumab or ipilimumab was assigned.
Results: In our search of 3,763 patients, 35 patients (0.93%) presented with 43 serious neurologic irAEs, including neuropathy (n = 22), noninfective meningitis (n = 5), encephalitis (n = 6), neuromuscular disorders (n = 3), and nonspecific adverse events (n = 7). Study drug was discontinued (n = 20), interrupted (n = 8), or unchanged (n = 7). Most neurologic irAEs resolved (26/35 patients; 75%). Overall, median time to onset was 45 days (range 1-170) and to resolution was 32 days (2-809+). Median time to onset of encephalitis was 55.5 days (range 18-297); four cases resolved and one was fatal.
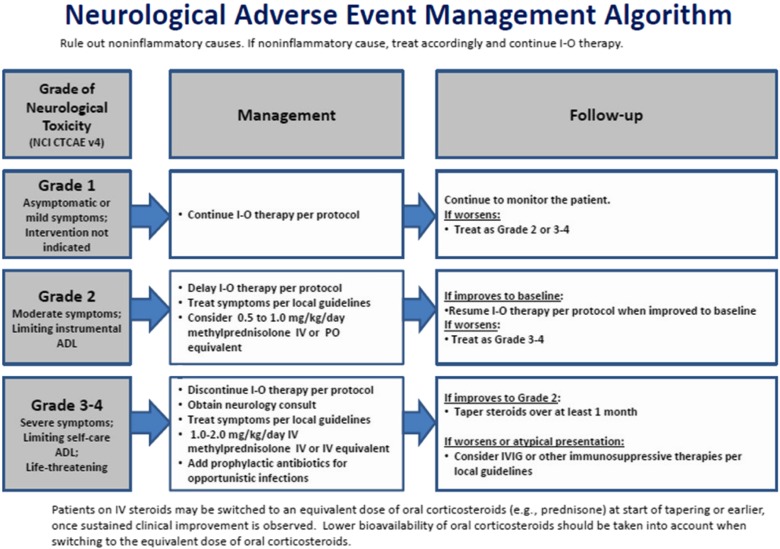
Conclusion: Both oncologists and neurologists need to be aware of signs and symptoms of serious but uncommon neurologic irAEs associated with checkpoint inhibitors. Prompt diagnosis and management using an established algorithm are critical to minimize serious complications from these neurologic irAEs.
Implications for practice: With increasing use of checkpoint inhibitors in cancer, practicing oncologists need to be aware of the potential risk of neurologic immune-related adverse events and be able to provide prompt treatment of this uncommon, but potentially serious, class of adverse events. We summarize neurologic adverse events related to nivolumab alone or in combination with ipilimumab in patients with advanced melanoma from 12 studies and examine in depth 6 cases of encephalitis. We also provide input and guidance on the existing neurologic adverse events management algorithm for nivolumab and ipilimumab.
Keywords: Case series; Encephalitis; Immune checkpoint inhibitors; Immune‐related adverse events; Melanoma; Neurologic adverse events.
© AlphaMed Press 2017.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Robert C, Long GV, Brady B et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med 2015;372:320–330. - PubMed
-
- Robert C, Schachter J, Long GV et al. Pembrolizumab versus ipilimumab in advanced melanoma. N Engl J Med 2015;372:2521–2532. - PubMed
-
- Weber JS, D'Angelo SP, Minor D et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti‐CTLA‐4 treatment (CheckMate 037): A randomised, controlled, open‐label, phase 3 trial. Lancet Oncol 2015;16:375–384. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
