

Lower-body negative pressure decreases noninvasively measured intracranial pressure and internal jugular vein cross-sectional area during head-down tilt
- PMID: 28495841
- PMCID: PMC5538811
- DOI: 10.1152/japplphysiol.00091.2017
Lower-body negative pressure decreases noninvasively measured intracranial pressure and internal jugular vein cross-sectional area during head-down tilt
Abstract
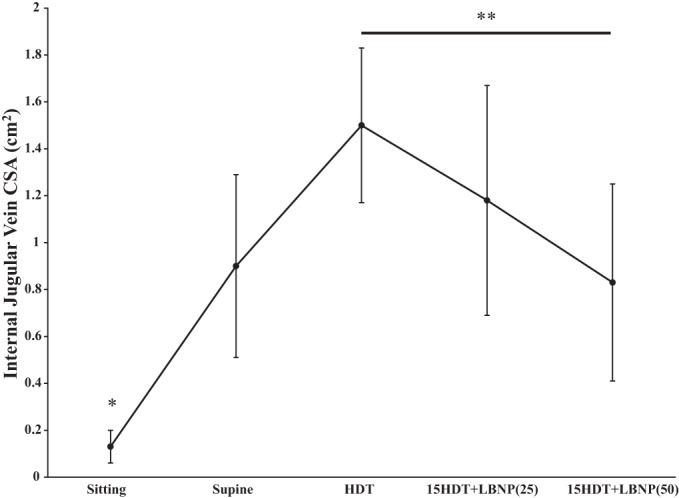
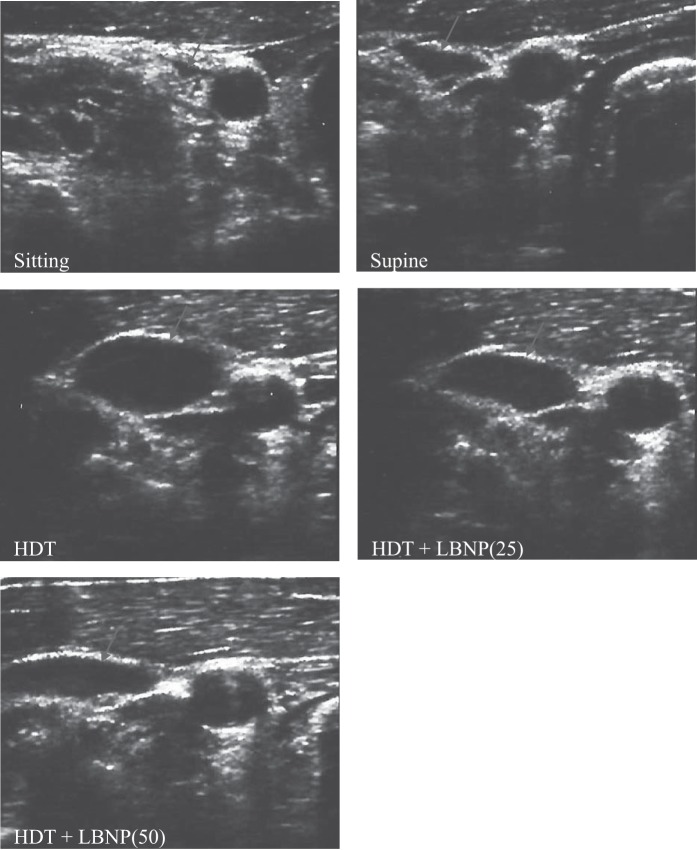
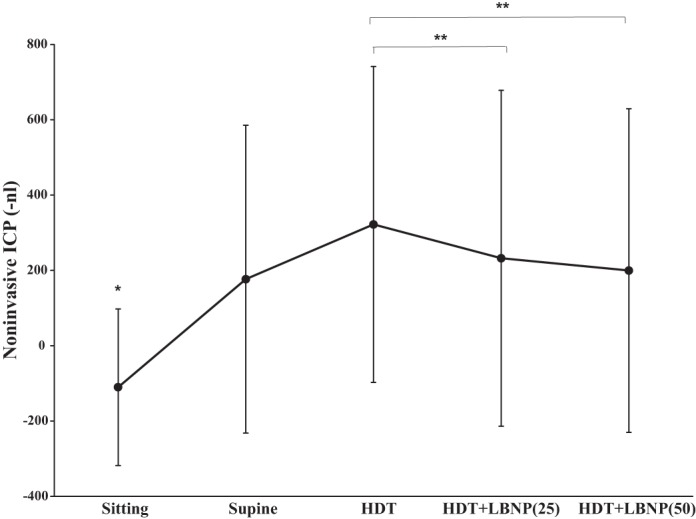
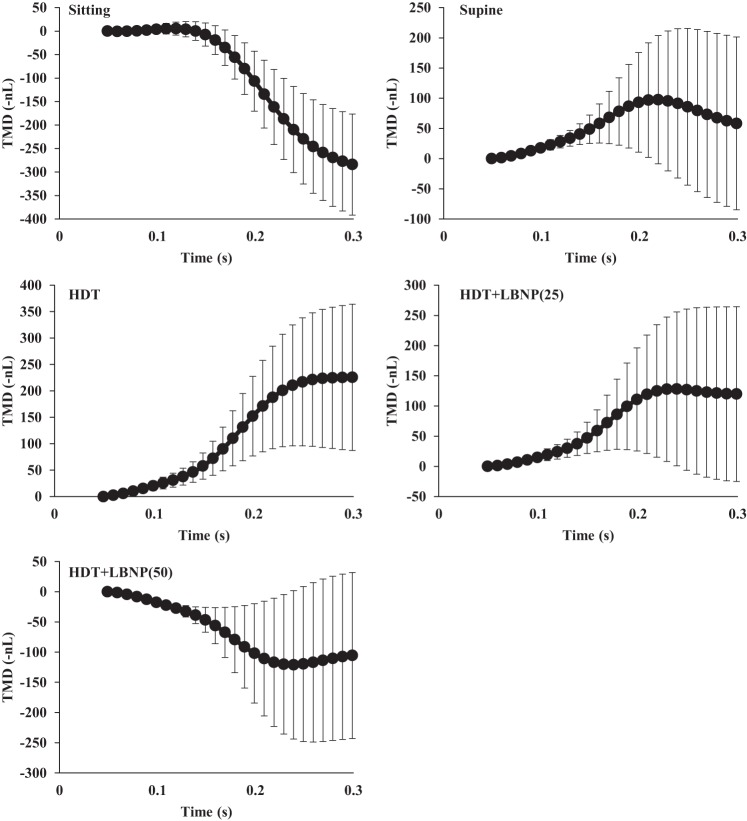
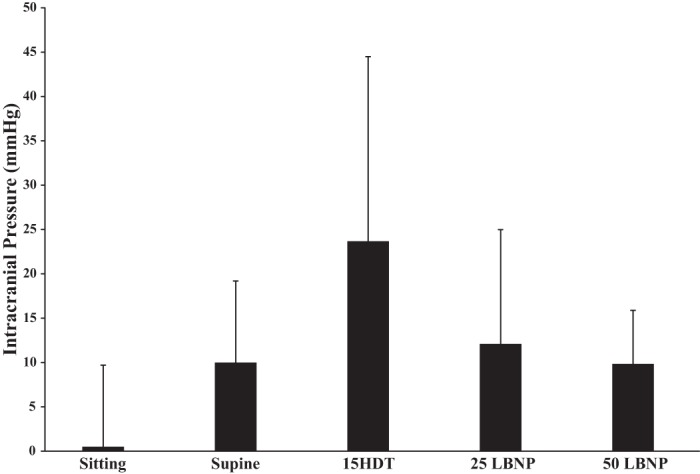
Long-term spaceflight induces a near visual acuity change in ~50% of astronauts. In some crew members, postflight cerebrospinal fluid (CSF) opening pressures by lumbar puncture are as high as 20.9 mmHg; these members demonstrated optic disc edema. CSF communicates through the cochlear aqueduct to affect perilymphatic pressure and tympanic membrane motion. We hypothesized that 50 mmHg of lower-body negative pressure (LBNP) during 15° head-down tilt (HDT) would mitigate elevations in internal jugular vein cross-sectional area (IJV CSA) and intracranial pressure (ICP). Fifteen healthy adult volunteers were positioned in sitting (5 min), supine (5 min), 15° HDT (5 min), and 15° HDT with LBNP (10 min) postures for data collection. Evoked tympanic membrane displacements (TMD) quantified ICP noninvasively. IJV CSA was measured using standard ultrasound techniques. ICP and IJV CSA increased significantly from the seated upright to the 15° HDT posture (P < 0.05), and LBNP mitigated these increases. LBNP at 25 mmHg reduced ICP during HDT (TMD of 322.13 ± 419.17 nl) to 232.38 ± 445.85 nl, and at 50 mmHg ICP was reduced further to TMD of 199.76 ± 429.69 nl. In addition, 50 mmHg LBNP significantly reduced IJV CSA (1.50 ± 0.33 cm2) during 15° HDT to 0.83 ± 0.42 cm2 LBNP counteracts the headward fluid shift elevation of ICP and IJV CSA experienced during microgravity as simulated by15° HDT. These data provide quantitative evidence that LBNP shifts cephalic fluid to the lower body, reducing IJV CSA and ICP.NEW & NOTEWORTHY The current study provides new evidence that 25 or 50 mmHg of lower body negative pressure reduces jugular venous pooling and intracranial pressure during simulated microgravity. Therefore, spaceflight countermeasures that sequester fluid to the lower body may mitigate cephalic venous congestion and vision impairment.
Keywords: spaceflight; tympanic membrane displacement; venous congestion; vision.
Copyright © 2017 the American Physiological Society.
Figures
References
-
- Arbeille P, Provost R, Zuj K, Vincent N. Measurements of jugular, portal, femoral, and calf vein cross-sectional area for the assessment of venous blood redistribution with long duration spaceflight (vessel imaging experiment). Eur J Appl Physiol 115: 2099–2106, 2015. doi: 10.1007/s00421-015-3189-6. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources