

The impact of ocular hemodynamics and intracranial pressure on intraocular pressure during acute gravitational changes
- PMID: 28495842
- PMCID: PMC5614788
- DOI: 10.1152/japplphysiol.00102.2017
The impact of ocular hemodynamics and intracranial pressure on intraocular pressure during acute gravitational changes
Abstract
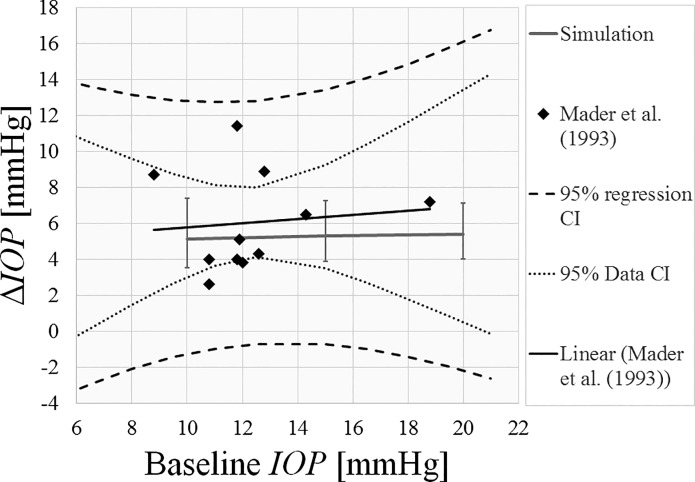
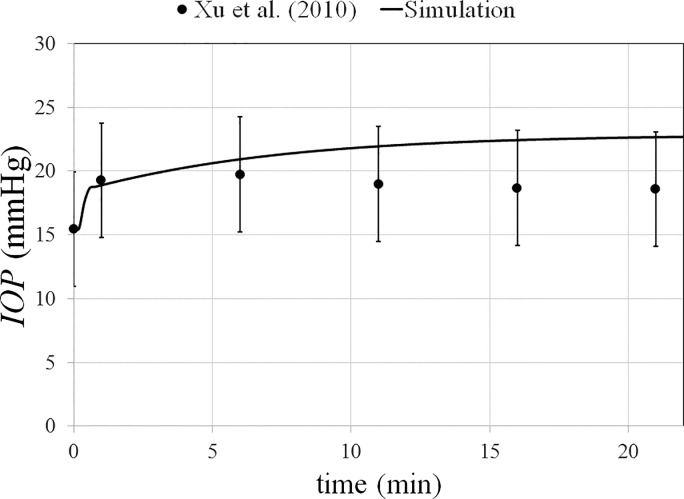
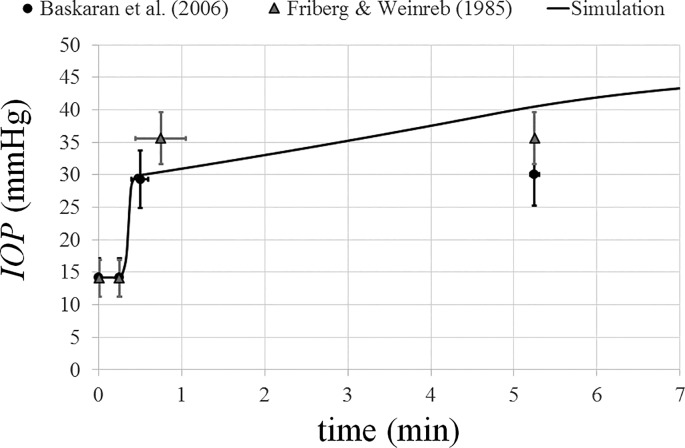
Exposure to microgravity causes a bulk fluid shift toward the head, with concomitant changes in blood volume/pressure, and intraocular pressure (IOP). These and other factors, such as intracranial pressure (ICP) changes, are suspected to be involved in the degradation of visual function and ocular anatomical changes exhibited by some astronauts. This is a significant health concern. Here, we describe a lumped-parameter numerical model to simulate volume/pressure alterations in the eye during gravitational changes. The model includes the effects of blood and aqueous humor dynamics, ICP, and IOP-dependent ocular compliance. It is formulated as a series of coupled differential equations and was validated against four existing data sets on parabolic flight, body inversion, and head-down tilt (HDT). The model accurately predicted acute IOP changes in parabolic flight and HDT, and was satisfactory for the more extreme case of inversion. The short-term response to the changing gravitational field was dominated by ocular blood pressures and compliance, while longer-term responses were more dependent on aqueous humor dynamics. ICP had a negligible effect on acute IOP changes. This relatively simple numerical model shows promising predictive capability. To extend the model to more chronic conditions, additional data on longer-term autoregulation of blood and aqueous humor dynamics are needed.NEW & NOTEWORTHY A significant percentage of astronauts present anatomical changes in the posterior eye tissues after spaceflight. Hypothesized increases in ocular blood volume and intracranial pressure (ICP) in space have been considered to be likely factors. In this work, we provide a novel numerical model of the eye that incorporates ocular hemodynamics, gravitational forces, and ICP changes. We find that changes in ocular hemodynamics govern the response of intraocular pressure during acute gravitational change.
Keywords: intracranial pressure; intraocular pressure; ocular blood flow; ocular compliance; space physiology; visual impairment and intracranial pressure.
Copyright © 2017 the American Physiological Society.
Figures









Similar articles
-
Intracranial and Intraocular Pressure During Various Degrees of Head-Down Tilt.Aerosp Med Hum Perform. 2017 Jan 1;88(1):10-16. doi: 10.3357/AMHP.4653.2017. Aerosp Med Hum Perform. 2017. PMID: 28061916
-
Increased cerebral blood volume pulsatility during head-down tilt with elevated carbon dioxide: the SPACECOT Study.J Appl Physiol (1985). 2017 Jul 1;123(1):62-70. doi: 10.1152/japplphysiol.00947.2016. Epub 2017 Mar 30. J Appl Physiol (1985). 2017. PMID: 28360122
-
Effects of short-term mild hypercapnia during head-down tilt on intracranial pressure and ocular structures in healthy human subjects.Physiol Rep. 2017 Jun;5(11):e13302. doi: 10.14814/phy2.13302. Physiol Rep. 2017. PMID: 28611153 Free PMC article.
-
The effect of microgravity on ocular structures and visual function: a review.Surv Ophthalmol. 2013 Mar-Apr;58(2):155-63. doi: 10.1016/j.survophthal.2012.04.002. Epub 2013 Jan 29. Surv Ophthalmol. 2013. PMID: 23369516 Review.
-
Spaceflight-Induced Intracranial Hypertension and Visual Impairment: Pathophysiology and Countermeasures.Physiol Rev. 2018 Jan 1;98(1):59-87. doi: 10.1152/physrev.00017.2016. Physiol Rev. 2018. PMID: 29167331 Review.
Cited by
-
Neurodegenerative Disorders of the Eye and of the Brain: A Perspective on Their Fluid-Dynamical Connections and the Potential of Mechanism-Driven Modeling.Front Neurosci. 2020 Nov 12;14:566428. doi: 10.3389/fnins.2020.566428. eCollection 2020. Front Neurosci. 2020. PMID: 33281543 Free PMC article. Review.
-
Evidence of Spaceflight-Induced Adverse Effects on Photoreceptors and Retinal Function in the Mouse Eye.Int J Mol Sci. 2023 Apr 17;24(8):7362. doi: 10.3390/ijms24087362. Int J Mol Sci. 2023. PMID: 37108526 Free PMC article.
-
Identifying the Critical Factors Governing Translaminar Pressure Differential Through a Compartmental Model.Invest Ophthalmol Vis Sci. 2019 Jul 1;60(8):3204-3214. doi: 10.1167/iovs.18-26200. Invest Ophthalmol Vis Sci. 2019. PMID: 31335946 Free PMC article.
-
Spaceflight influences gene expression, photoreceptor integrity, and oxidative stress-related damage in the murine retina.Sci Rep. 2019 Sep 16;9(1):13304. doi: 10.1038/s41598-019-49453-x. Sci Rep. 2019. PMID: 31527661 Free PMC article.
-
Effect of Muslim Prayer (Salat) positions on the intra-ocular pressure in healthy young individuals.Indian J Ophthalmol. 2023 Jun;71(6):2495-2499. doi: 10.4103/IJO.IJO_2565_22. Indian J Ophthalmol. 2023. PMID: 37322669 Free PMC article.
References
-
- Alexander DJ, Gibson CR, Hamilton DR, Lee SMC, Mader TH, Otto C, Oubre CM, Pass AF, Platts S, Scott JM, Smith SM, Stenger MB, Westby CM, Zanello SB. Evidence Report: Risk of Spaceflight-Induced Intracranial Hypertension and Vision Alterations. Washington, DC: NASA, 2012.
-
- Ansari R, Suh KI, Moret F, Messer RK, Manuel FK. Measurement of choroidal blood flow in zero gravity. In: Opthalmic Technologies XIII (Manns F, Soderberg PG, Ho ASPIE, Eds.). 2003, p. 177–184. doi:10.1117/12.479427 - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources