

Longitudinal fluorescence in situ hybridization reveals cytogenetic evolution in myeloma relapsing after autologous transplantation
- PMID: 28495913
- PMCID: PMC5541876
- DOI: 10.3324/haematol.2017.168005
Longitudinal fluorescence in situ hybridization reveals cytogenetic evolution in myeloma relapsing after autologous transplantation
Abstract
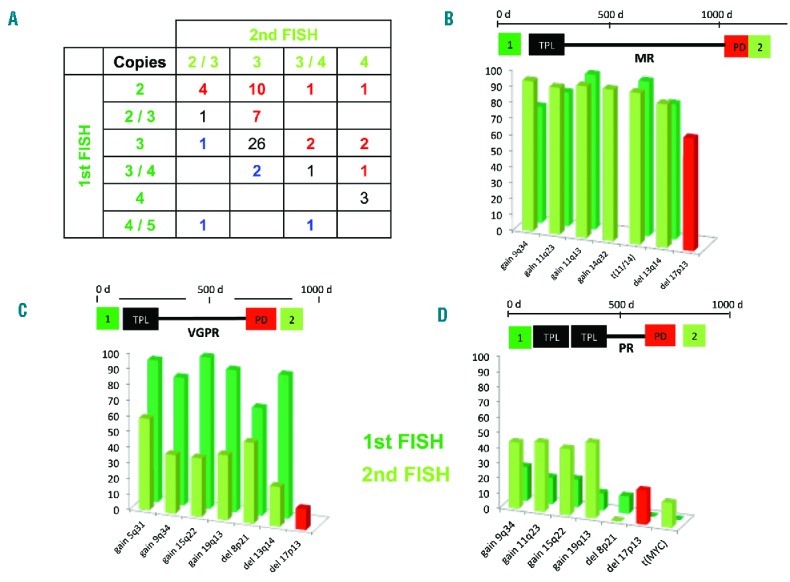
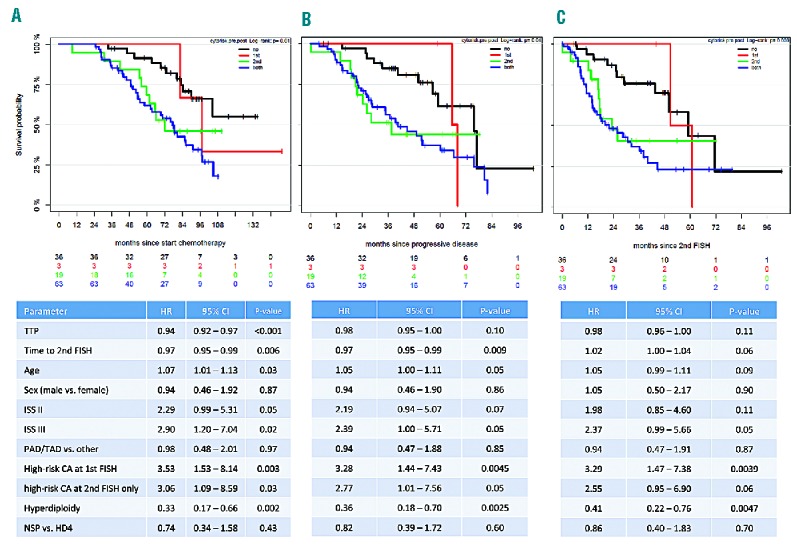
To investigate cytogenetic evolution after upfront autologous stem cell transplantation for newly diagnosed myeloma we retrospectively analyzed fluorescence in situ hybridization results of 128 patients with paired bone marrow samples from the time of primary diagnosis and at relapse. High-risk cytogenetic abnormalities (deletion 17p and/or gain 1q21) occurred more frequently after relapse (odds ratio: 6.33; 95% confidence interval: 1.86-33.42; P<0.001). No significant changes were observed for defined IGH translocations [t(4;14); t(11;14); t(14;16)] or hyperdiploid karyotypes between primary diagnosis and relapse. IGH translocations with unknown partners occurred more frequently at relapse. New deletion 17p and/or gain 1q21 were associated with cytogenetic heterogeneity, since some de novo lesions with different copy numbers were present only in subclones. No distinct baseline characteristics were associated with the occurrence of new high-risk cytogenetic abnormalities after progression. Patients who relapsed after novel agent-based induction therapy had an increased risk of developing high-risk aberrations (odds ratio 10.82; 95% confidence interval: 1.65-127.66; P=0.03) compared to those who were treated with conventional chemotherapy. Survival analysis revealed dismal outcomes regardless of whether high-risk aberrations were present at baseline (hazard ratio, 3.53; 95% confidence interval: 1.53-8.14; P=0.003) or developed at relapse only (hazard ratio, 3.06; 95% confidence interval: 1.09-8.59; P=0.03). Our results demonstrate cytogenetic evolution towards high-risk disease after autologous transplantation and underline the importance of repeated genetic testing in relapsed myeloma (EudraCT number of the HD4 trial: 2004-000944-26).
Copyright© 2017 Ferrata Storti Foundation.
Figures
References
-
- Manier S, Salem KZ, Park J, Landau DA, Getz G, Ghobrial IM. Genomic complexity of multiple myeloma and its clinical implications. Nat Rev Clin Oncol. 2017;14(2):100–113. - PubMed
-
- Morgan GJ, Walker BA, Davies FE. The genetic architecture of multiple myeloma. Nat Rev Cancer. 2012;12(5):335–348. - PubMed
-
- Moreau P, Cavo M, Sonneveld P, et al. Combination of international scoring system 3, high lactate dehydrogenase, and t(4;14) and/or del(17p) identifies patients with multiple myeloma (MM) treated with front-line autologous stem-cell transplantation at high risk of early MM progression-related death. J Clin Oncol. 2014;32(20):2173–2180. - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
