

TIPIC Syndrome: Beyond the Myth of Carotidynia, a New Distinct Unclassified Entity
- PMID: 28495942
- PMCID: PMC7959891
- DOI: 10.3174/ajnr.A5214
TIPIC Syndrome: Beyond the Myth of Carotidynia, a New Distinct Unclassified Entity
Abstract
Background and purpose: The differential diagnosis of acute cervical pain includes nonvascular and vascular causes such as carotid dissection, carotid occlusion, or vasculitis. However, some patients present with unclassified vascular and perivascular changes on imaging previously reported as carotidynia. The aim of our study was to improve the description of this as yet unclassified clinico-radiologic entity.
Materials and methods: From January 2009 through April 2016, 47 patients from 10 centers presenting with acute neck pain or tenderness and at least 1 cervical image showing unclassified carotid abnormalities were included. We conducted a systematic, retrospective study of their medical charts and diagnostic and follow-up imaging. Two neuroradiologists independently analyzed the blinded image datasets.
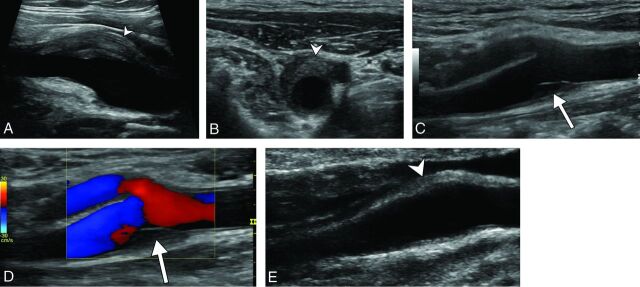
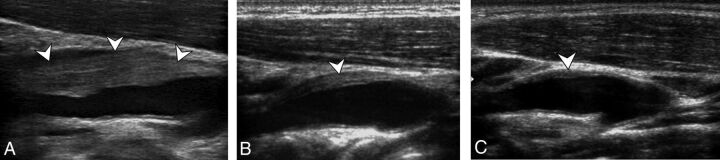
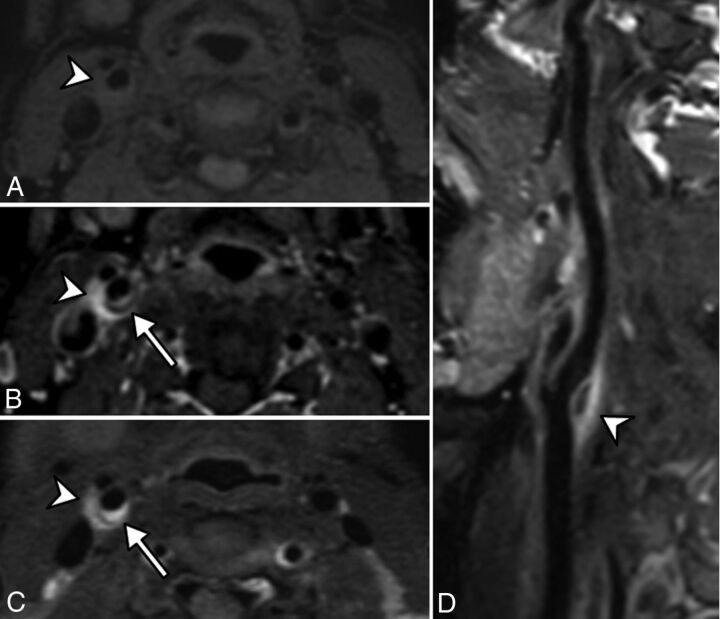
Results: The median patient age was 48 years. All patients presented with acute neck pain, and 8 presented with transient neurologic symptoms. Imaging showed an eccentric pericarotidian infiltration in all patients. An intimal soft plaque was noted in 16 patients, and a mild luminal narrowing was noted in 16 patients. Interreader reproducibility was excellent. All patients had complete pain resolution within a median of 13 days. At 3-month follow-up, imaging showed complete disappearance of vascular abnormalities in 8 patients, and a marked decrease in all others.
Conclusions: Our study improved the description of an unclassified, clinico-radiologic entity, which could be described by the proposed acronym: TransIent Perivascular Inflammation of the Carotid artery (TIPIC) syndrome.
© 2017 by American Journal of Neuroradiology.
Figures

Comment in
-
TransIent Perivascular Inflammation of the Carotid artery syndrome: TIPIC, a new clinical entity that must be recognised by ENT surgeons.Eur Ann Otorhinolaryngol Head Neck Dis. 2020 Jan;137(1):87-88. doi: 10.1016/j.anorl.2019.10.001. Epub 2019 Dec 10. Eur Ann Otorhinolaryngol Head Neck Dis. 2020. PMID: 31836495 No abstract available.
References
-
- Fay T. Atypical neuralgia. Arch Neurol Psychiatry 1927;18:309–15
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous