

Prospective evaluation of intense pulsed light and meibomian gland expression efficacy on relieving signs and symptoms of dry eye disease due to meibomian gland dysfunction
- PMID: 28496300
- PMCID: PMC5422561
- DOI: 10.2147/OPTH.S130706
Prospective evaluation of intense pulsed light and meibomian gland expression efficacy on relieving signs and symptoms of dry eye disease due to meibomian gland dysfunction
Abstract
Purpose: The aim of this study was to estimate the efficacy of intense pulsed light (IPL), followed by meibomian gland expression (MGX), for reducing the number and severity of signs and symptoms of dry eye disease (DED) secondary to meibomian gland dysfunction (MGD).
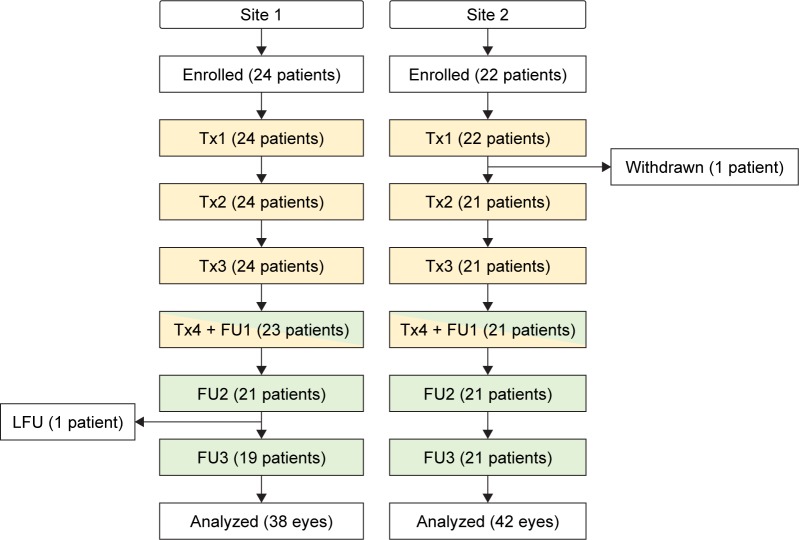
Patients and methods: In a prospective study conducted in two sites, 40 subjects (80 eyes) with moderate to severe MGD were enrolled. Major inclusion criteria consisted of at least two of the following measures being compatible with DED in both eyes: tear breakup time (TBUT), meibomian gland score (MGS), corneal fluorescein staining (CFS), Standard Patient Evaluation of Eye Dryness (SPEED) questionnaire, and tear film osmolarity (TFO). Enrolled patients underwent four treatment sessions, 3 weeks apart. Each treatment included the administration of 10-15 pulses of IPL on the cheeks and nose, followed by MGX of the upper and lower eyelids. TBUT, MGS, CFS, SPEED, TFO, and lipid layer thickness (LLT) were measured at baseline (BL) and at 9, 12, and 15 weeks after BL.
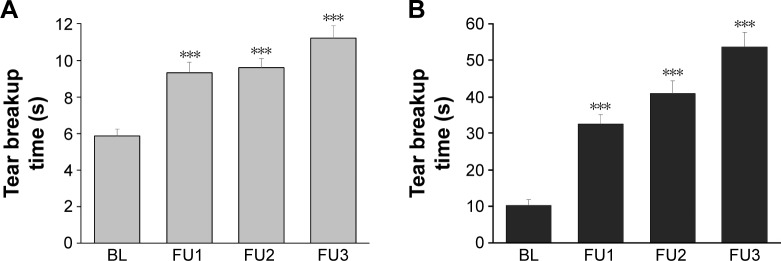
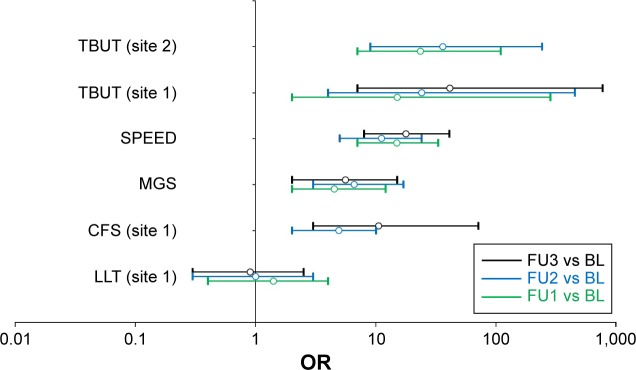
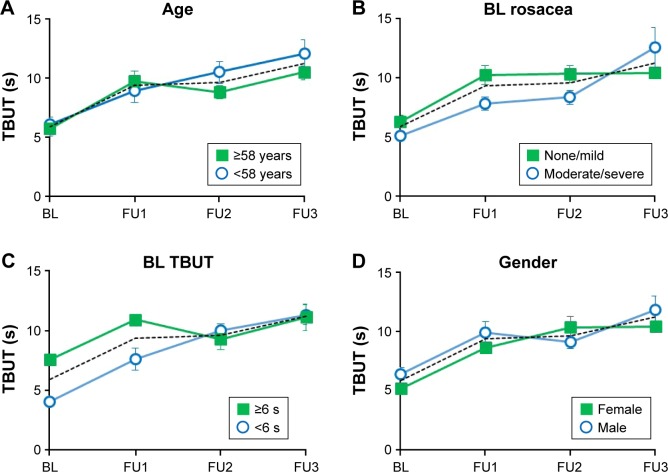
Results: Due to different staining methods used for TBUT measurements, TBUT and CFS were analyzed separately for each site. From BL to the final follow-up, the number of signs compatible with DED decreased from 3.3±0.1 to 1.4±0.1. TBUT improved by +93% (n=38; P<0.0001) and +425% (n=42; P<0.0001) for sites 1 and 2, respectively. SPEED, MGS, and CFS improved by -55% (n=80; P<0.0001), -36% (n=80; P<0.0001), and -58% (n=38; P<0.0001), respectively. In 20 eyes with abnormally elevated TFO at BL, TFO improved by -7% (n=20; P<0.005). LLT did not change (n=38; P=0.88).
Conclusion: In subjects with moderate to severe MGD, IPL combined with MGX reduced the number and severity of symptoms and signs of DED. Except for LLT, all examined outcome measures significantly improved after 15 weeks. These results support the efficacy of IPL + MGX in relieving both signs and symptoms of DED secondary to MGD.
Keywords: dry eye; intense pulsed light; meibomian gland dysfunction.
Conflict of interest statement
Disclosure SJD, RNG, SCB, and DNC are consultants to Lumenis. The authors report no other conflicts of interest in this work.
Figures
References
-
- Lemp MA, Crews LA, Bron AJ, Foulks GN, Sullivan BD. Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort. Cornea. 2012;31(5):472–478. - PubMed
-
- Akpek EK, Merchant A, Pinar V, Foster CS. Ocular rosacea: patient characteristics and follow up. Ophthalmology. 1997;104(11):1863–1867. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
