

Surgical Treatment of Atrial Fibrillation
- PMID: 28496568
- PMCID: PMC5398793
- DOI: 10.4022/jafib.19
Surgical Treatment of Atrial Fibrillation
Abstract
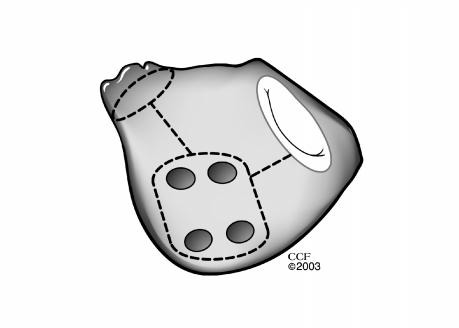
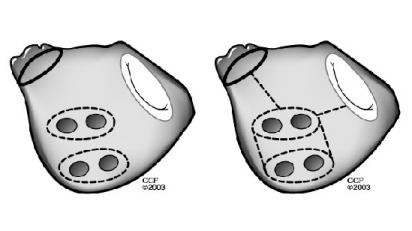
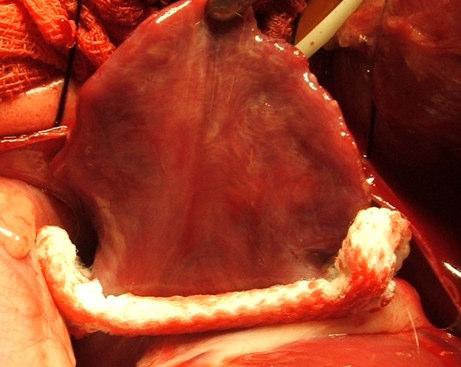
Atrial fibrillation (AF) is now commonly treated at the time of valvular heart surgery or coronary artery bypass grafting. Surgical ablation of AF, which is predicated upon the Maze procedure, includes creation of lines of conduction block and excision of the left atrial appendage. A full bi-atrial lesion set is associated with success in 80% to 95% of patients and virtually eliminates the risk of late stroke. A complex but safe operation, the classic cut-and-sew Maze procedure has been applied by relatively few surgeons. However, recent advances in understanding of the pathogenesis of AF and development of new ablation technologies enable surgeons to perform pulmonary vein isolation, create linear left and right atrial lesions, and remove the left atrial appendage rapidly and safely. Lesions are created under direct vision, minimizing the risk of damage to the pulmonary veins and adjacent mediastinal structures. Recently developed instrumentation now enables thoracoscopic and keyhole approaches, facilitating extension of epicardial AF ablation and excision of the left atrial appendage to patients with isolated AF and no other indication for cardiac surgery. In addition, novel devices designed specifically for minimally invasive epicardial exclusion of the left atrial appendage will broaden the range of treatment options for patients with AF, possibly eliminating the need for anticoagulation in selected patients.
Figures
References
-
- Haïssaguerre M, Jaïs P, Shah D C, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Métayer P, Clémenty J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N. Engl. J. Med. 1998 Sep 03;339 (10):659–66. - PubMed
-
- Jaïs P, Haïssaguerre M, Shah D C, Chouairi S, Gencel L, Hocini M, Clémenty J. A focal source of atrial fibrillation treated by discrete radiofrequency ablation. Circulation. 1997 Feb 04;95 (3):572–6. - PubMed
-
- Chen S A, Hsieh M H, Tai C T, Tsai C F, Prakash V S, Yu W C, Hsu T L, Ding Y A, Chang M S. Initiation of atrial fibrillation by ectopic beats originating from the pulmonary veins: electrophysiological characteristics, pharmacological responses, and effects of radiofrequency ablation. Circulation. 1999 Nov 02;100 (18):1879–86. - PubMed
-
- Lu T M, Tai C T, Hsieh M H, Tsai C F, Lin Y K, Yu W C, Tsao H M, Lee S H, Ding Y A, Chang M S, Chen S A. Electrophysiologic characteristics in initiation of paroxysmal atrial fibrillation from a focal area. J. Am. Coll. Cardiol. 2001 May;37 (6):1658–64. - PubMed
-
- Davidenko J M, Pertsov A V, Salomonsz R, Baxter W, Jalife J. Stationary and drifting spiral waves of excitation in isolated cardiac muscle. Nature. 1992 Jan 23;355 (6358):349–51. - PubMed
Publication types
LinkOut - more resources
Full Text Sources