

Characterization of Left Atrial Tachyarrhythmias in Patients Following Atrial Fibrillation Ablation:Correlation of surface ECG with Intracardiac Mapping
- PMID: 28496571
- PMCID: PMC5398796
- DOI: 10.4022/jafib.27
Characterization of Left Atrial Tachyarrhythmias in Patients Following Atrial Fibrillation Ablation:Correlation of surface ECG with Intracardiac Mapping
Abstract
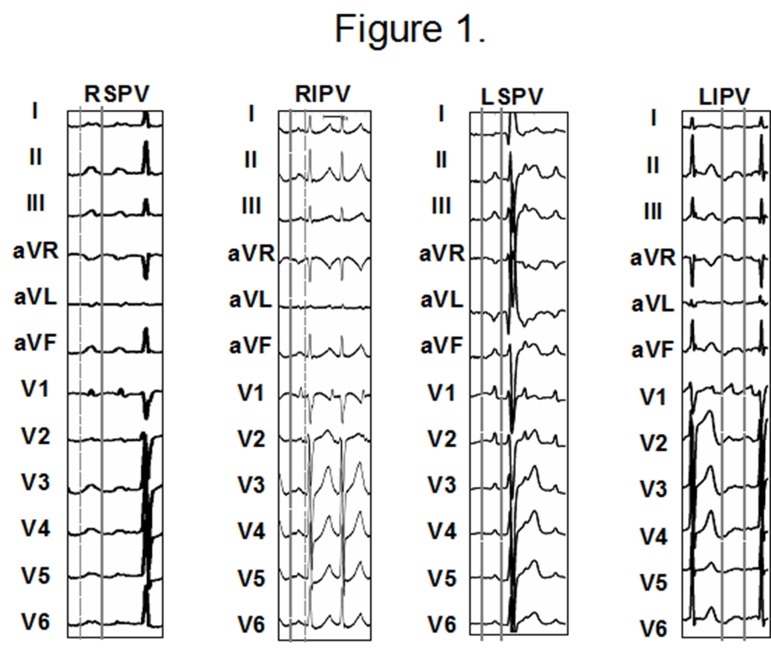
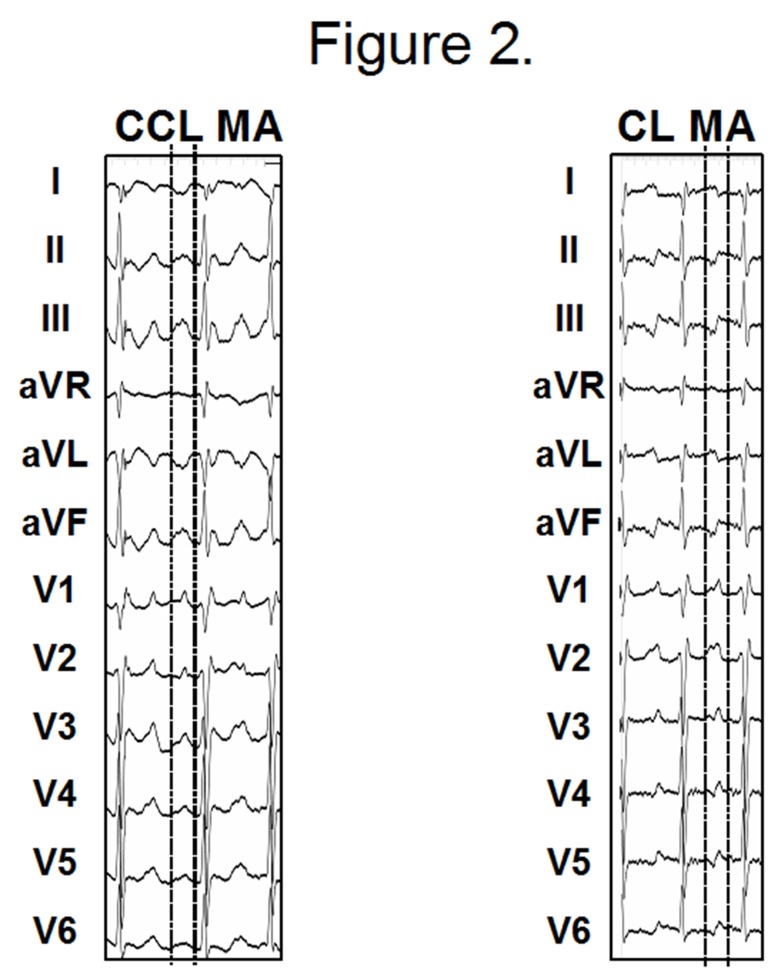
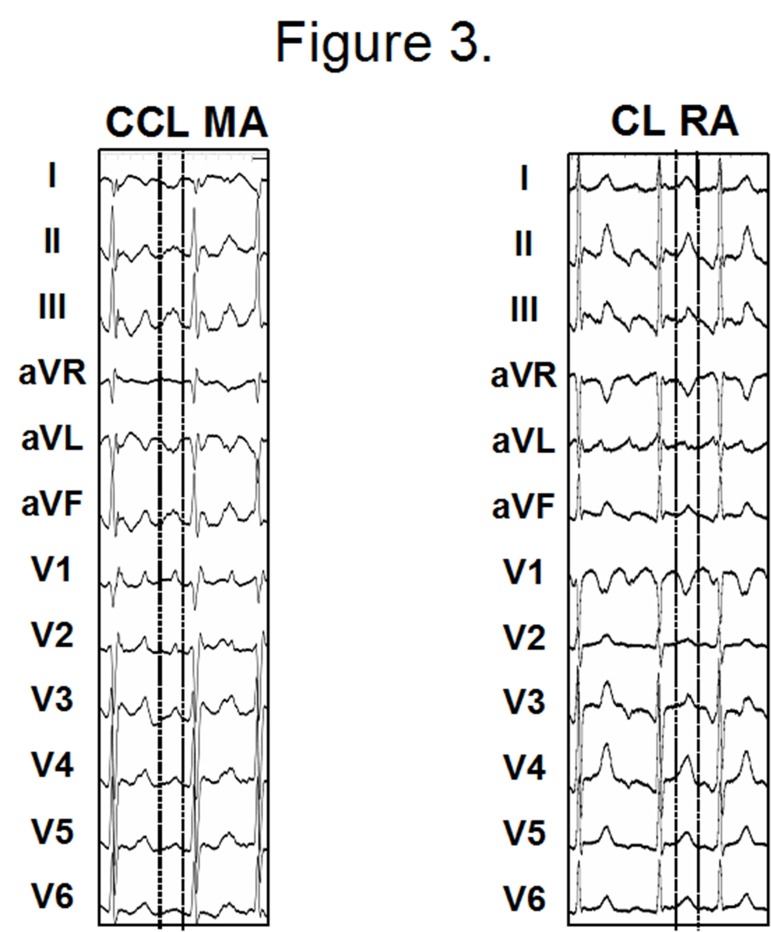
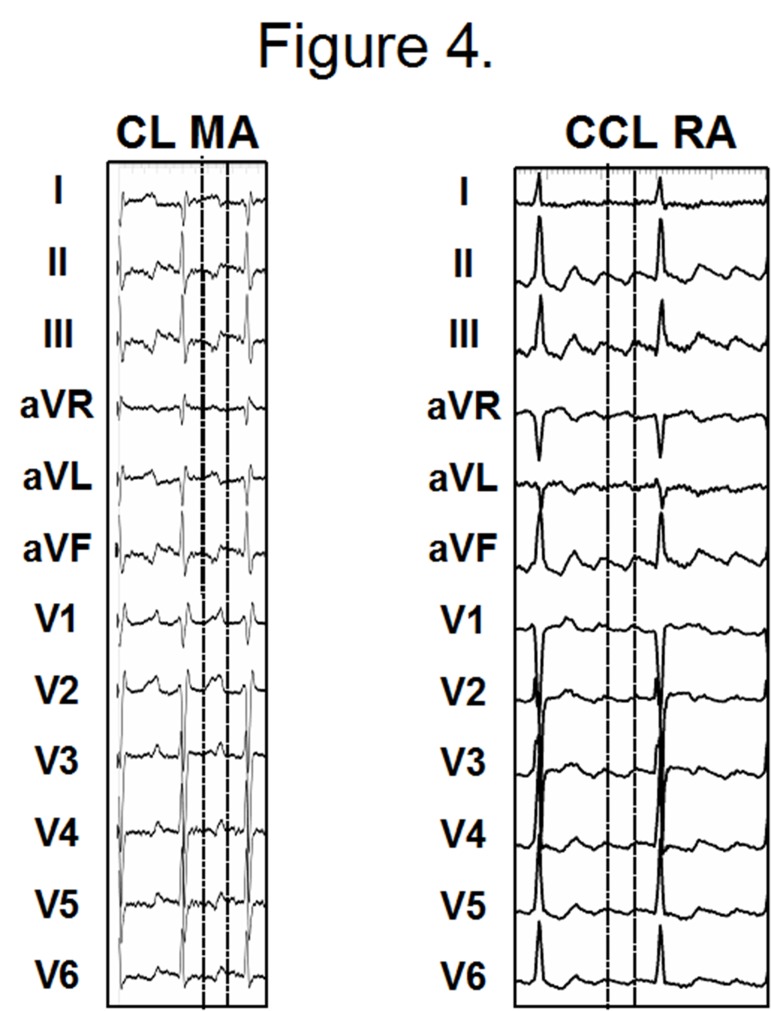
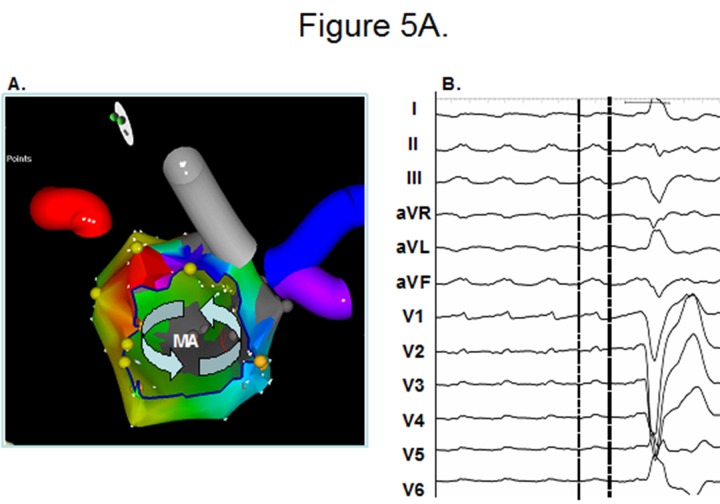
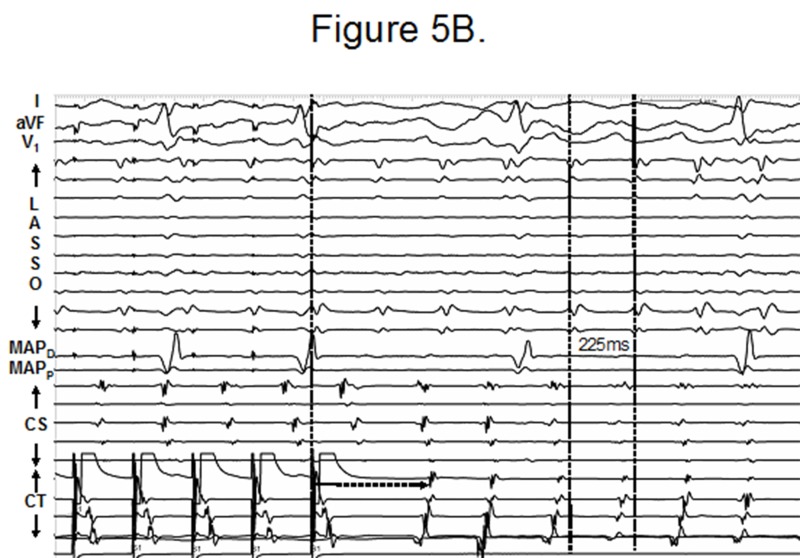
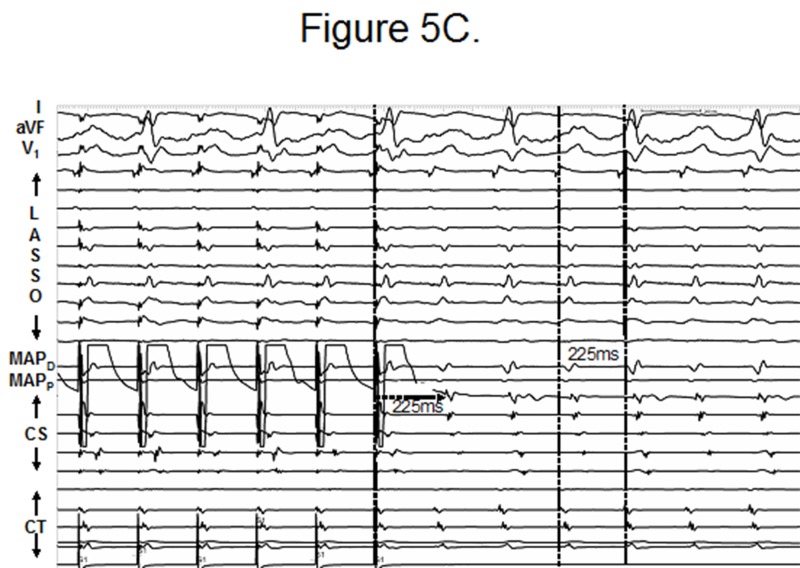
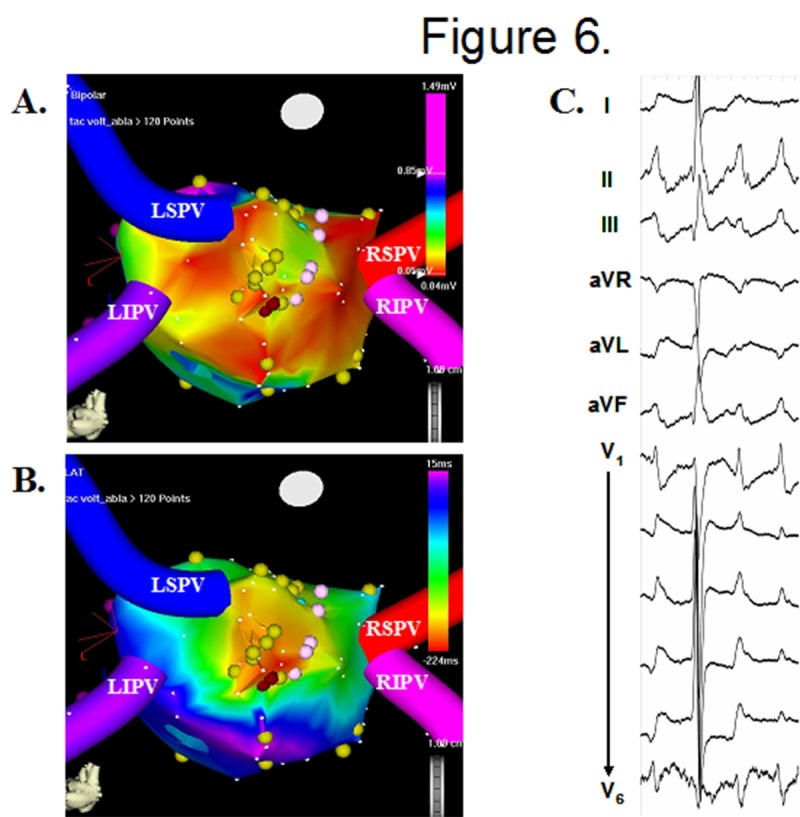
With expected success rates in excess of 80% for achieving long term arrhythmia control, catheter based ablation has become a popular treatment strategy in the management of patients with atrial fibrillation (AF). However, the success of AF ablation has been tempered by the occurrence of post procedure left atrial tachycardias and / or flutters, which can be seen in up to 30% of the patients. These arrhythmias are perpetuated either due to abnormalities of impulse formation (abnormal automaticity / triggered activity), or abnormalities of impulse conduction (micro / macroreentry). Regardless of the underlying mechanism, these tachycardias manifest distinct "P" or flutter waves on the surface ECG, recognition of which may facilitate their characterization / localization. However, because of the frequent overlap in the morphology of P waves, intracardiac mapping is often the only way to distinguish them apart. This is accomplished using a combination of activation, entrainment and electroanatomic mapping techniques. Tachycardias resulting from abnormalities of impulse formation and / or microreentry are characteristically focal and usually confined in and around pulmonary vein (PV) segments which have reconnected (septal aspect of right PVs and anterior aspect of left PVs). In contrast, macroreentrant tachycardias manifest a large circuit dimension involving zone(s) of slow conduction. These are most commonly seen to occur around the mitral valve but can develop in any part of the left atrium where "gaps" across prior ablation lesion sets create altered conduction. Successful ablation of focal tachycardias is usually accomplished by isolating the reconnected PV segment(s). In case of macroreentrant arrhythmias however, a more extensive ablation approach is typically required in order to achieve conduction block across isthmus of the circuit. Using these strategies, the majority of left atrial tachycardias occurring post AF ablation can be successfully cured with excellent long term results.
Figures
References
-
- Dixit Sanjay, Gerstenfeld Edward P, Ratcliffe Sarah J, Cooper Joshua M, Russo Andrea M, Kimmel Stephen E, Callans David J, Lin David, Verdino Ralph J, Patel Vickas V, Zado Erica, Marchlinski Francis E. Single procedure efficacy of isolating all versus arrhythmogenic pulmonary veins on long-term control of atrial fibrillation: a prospective randomized study. Heart Rhythm. 2008 Feb;5 (2):174–81. - PubMed
-
- Pappone Carlo, Manguso Francesco, Vicedomini Gabriele, Gugliotta Filippo, Santinelli Ornella, Ferro Amedeo, Gulletta Simone, Sala Simone, Sora Nicoleta, Paglino Gabriele, Augello Giuseppe, Agricola Eustachio, Zangrillo Alberto, Alfieri Ottavio, Santinelli Vincenzo. Prevention of iatrogenic atrial tachycardia after ablation of atrial fibrillation: a prospective randomized study comparing circumferential pulmonary vein ablation with a modified approach. Circulation. 2004 Nov 09;110 (19):3036–42. - PubMed
-
- Oral Hakan, Chugh Aman, Lemola Kristina, Cheung Peter, Hall Burr, Good Eric, Han Jihn, Tamirisa Kamala, Bogun Frank, Pelosi Frank, Morady Fred. Noninducibility of atrial fibrillation as an end point of left atrial circumferential ablation for paroxysmal atrial fibrillation: a randomized study. Circulation. 2004 Nov 02;110 (18):2797–801. - PubMed
-
- Cappato Riccardo, Calkins Hugh, Chen Shih-Ann, Davies Wyn, Iesaka Yoshito, Kalman Jonathan, Kim You-Ho, Klein George, Packer Douglas, Skanes Allan. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circulation. 2005 Mar 08;111 (9):1100–5. - PubMed
-
- Karch Martin R, Zrenner Bernhard, Deisenhofer Isabel, Schreieck Jürgen, Ndrepepa Gjin, Dong Jun, Lamprecht Katrin, Barthel Petra, Luciani Etienne, Schömig Albert, Schmitt Claus. Freedom from atrial tachyarrhythmias after catheter ablation of atrial fibrillation: a randomized comparison between 2 current ablation strategies. Circulation. 2005 Jun 07;111 (22):2875–80. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials