

Gender and Racial Characteristics of Patients Referred to a Tertiary Atrial Fibrillation Center
- PMID: 28496679
- PMCID: PMC5398821
- DOI: 10.4022/jafib.301
Gender and Racial Characteristics of Patients Referred to a Tertiary Atrial Fibrillation Center
Abstract
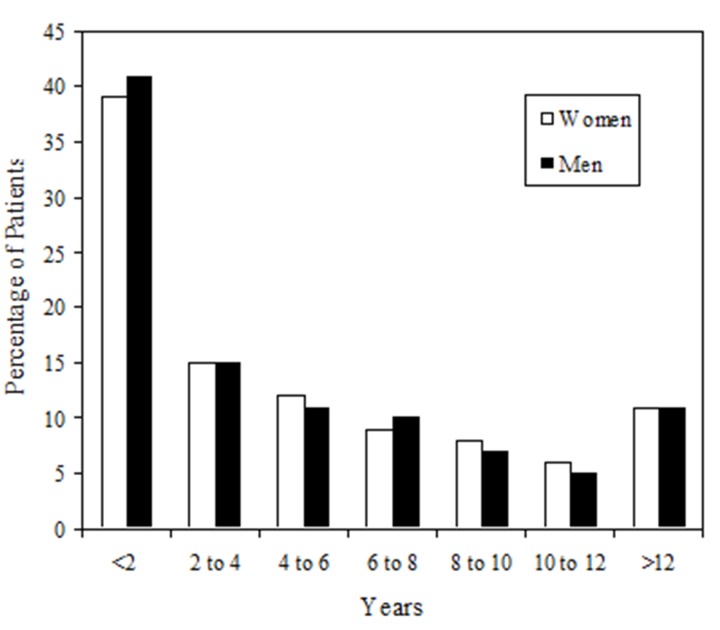
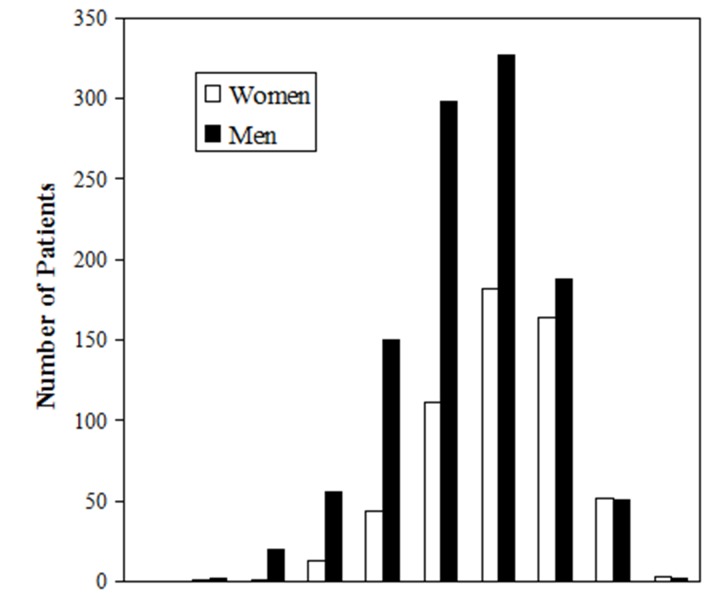
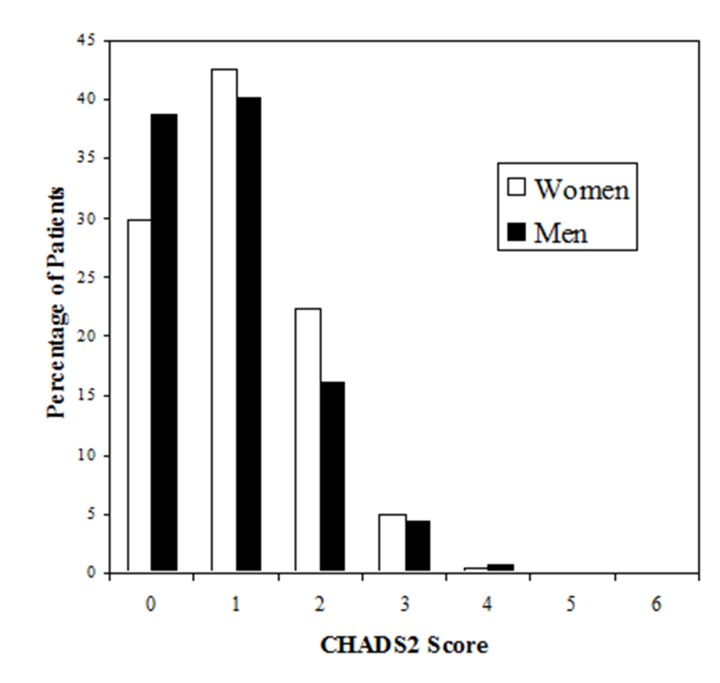
Atrial Fibrillation Centers (AFCs) are becoming increasingly common and are often developed at institutions to provide comprehensive evaluation and management for patients with atrial fibrillation (AF) including catheter and surgical ablation. Studies have shown that women and racial minority patients are less likely to be offered aggressive or invasive therapies. The University of Virginia (UVA) AFC was opened in 2004. We analyzed data collected during initial visits to our AFC from 2004-2008 to determine the gender and racial characteristics of a tertiary AFC population. Multivariable regression analysis was used to compare clinical characteristics. There were a total of 1664 consecutive initial patient visits. Cardiologists referred 61% and primary care physicians referred 37% of patients. Twice as many men were referred as women (570 vs. 1094; P<0.0001). Women were older (68.0±11.9 vs. 62.4±13.0 years; P<0.0001) and more symptomatic with palpitations (80% vs. 73%; P=0.008), but otherwise were not substantially different from men. Our referring physicians treated the majority of both men and women with anticoagulant and rate-controlling medications. African American patients accounted for 2.8% of AFC initial visits. In contrast, they accounted for 7.4% of patients seen for a primary diagnosis of AF at all other UVA outpatient clinics (P<0.0001). In conclusion, the demographics of a tertiary AFC are different than those of the general population. Women and racial minority patients are underrepresented, and the women have few comorbidities and symptoms than the known epidemiology would lead us to expect.
Figures
References
-
- Naccarelli Gerald V, Varker Helen, Lin Jay, Schulman Kathy L. Increasing prevalence of atrial fibrillation and flutter in the United States. Am. J. Cardiol. 2009 Dec 01;104 (11):1534–9. - PubMed
-
- Chen Lin Y, Shen Win-Kuang. Epidemiology of atrial fibrillation: a current perspective. Heart Rhythm. 2007 Mar;4 (3 Suppl):S1–6. - PubMed
-
- Cabin H S, Clubb K S, Hall C, Perlmutter R A, Feinstein A R. Risk for systemic embolization of atrial fibrillation without mitral stenosis. Am. J. Cardiol. 1990 May 01;65 (16):1112–6. - PubMed
-
- Benjamin E J, Wolf P A, D'Agostino R B, Silbershatz H, Kannel W B, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998 Sep 08;98 (10):946–52. - PubMed
LinkOut - more resources
Full Text Sources