

Review
doi: 10.4022/jafib.525.
eCollection 2012 Aug-Sep.
Post Ablation Left Atrial Tachycardia: Understanding Mechanism, Prevention and Treatment
Affiliations
- PMID: 28496760
- PMCID: PMC5153123
- DOI: 10.4022/jafib.525
Item in Clipboard
Review
Post Ablation Left Atrial Tachycardia: Understanding Mechanism, Prevention and Treatment
J Atr Fibrillation.
.
Abstract
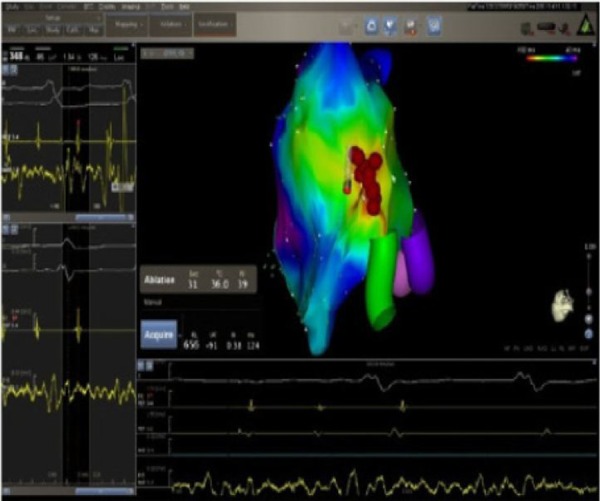
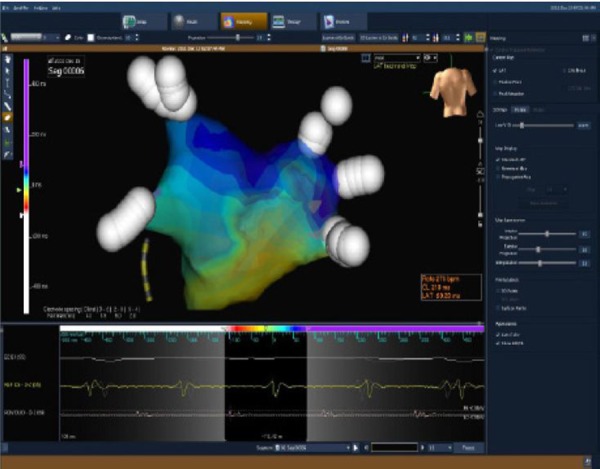
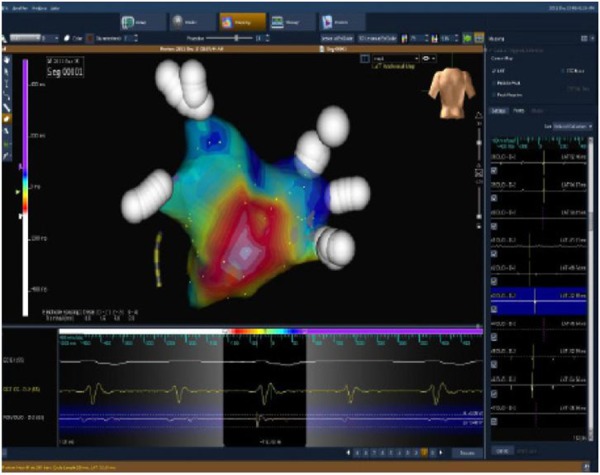
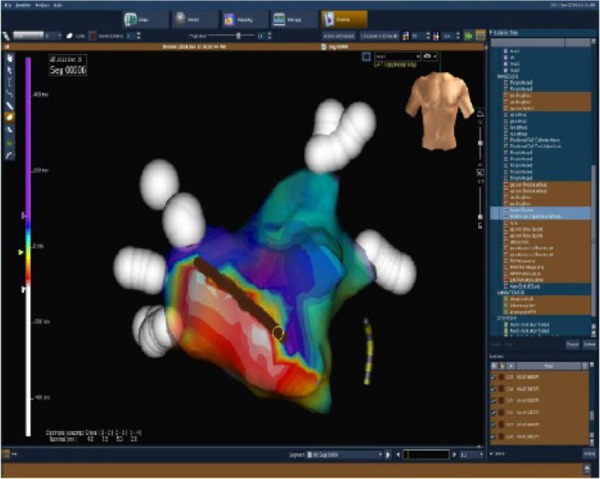
Currently, post-ablation Atrial Tachycardias (ATs) represent a growing clinical problem particularly in patients with persistent AF undergoing a more extensive substrate ablation. Understanding mechanisms and location of potentially widely located arrhythmogenic substrates in the left atrium is crucial for successful ablation. Mapping and ablation are challenging since complex and multiple ATs may frequently develop during the index procedure and before conversion to sinus rhythm. Use of irrigated ablation guided by detailed 3-D electroanatomic activation maps combined with entrainment pacing is effective with excellent acute and long-term success rates, rarely requiring multiple procedures.
Figures



References
-
- Wann L Samuel, Curtis Anne B, January Craig T, Ellenbogen Kenneth A, Lowe James E, Estes N A Mark, Page Richard L, Ezekowitz Michael D, Slotwiner David J, Jackman Warren M, Stevenson William G, Tracy Cynthia M, Fuster Valentin, Rydén Lars E, Cannom David S, Le Heuzey Jean-Yves, Crijns Harry J, Lowe James E, Curtis Anne B, Olsson S Bertil, Ellenbogen Kenneth A, Prystowsky Eric N, Halperin Jonathan L, Tamargo Juan Luis, Kay G Neal, Wann L Samuel, Jacobs Alice K, Anderson Jeffrey L, Albert Nancy, Hochman Judith S, Buller Christopher E, Kushner Frederick G, Creager Mark A, Ohman Erik Magnus, Ettinger Steven M, Stevenson William G, Guyton Robert A, Tarkington Lynn G, Halperin Jonathan L, Yancy Clyde W. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (Updating the 2006 Guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2011 Jan 11;57 (2):223–42. - PubMed
-
- Cappato Riccardo, Calkins Hugh, Chen Shih-Ann, Davies Wyn, Iesaka Yoshito, Kalman Jonathan, Kim You-Ho, Klein George, Packer Douglas, Skanes Allan. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circulation. 2005 Mar 08;111 (9):1100–5. - PubMed
-
- Pappone Carlo, Rosanio Salvatore, Augello Giuseppe, Gallus Giuseppe, Vicedomini Gabriele, Mazzone Patrizio, Gulletta Simone, Gugliotta Filippo, Pappone Alessia, Santinelli Vincenzo, Tortoriello Valter, Sala Simone, Zangrillo Alberto, Crescenzi Giuseppe, Benussi Stefano, Alfieri Ottavio. Mortality, morbidity, and quality of life after circumferential pulmonary vein ablation for atrial fibrillation: outcomes from a controlled nonrandomized long-term study. J. Am. Coll. Cardiol. 2003 Jul 16;42 (2):185–97. - PubMed
-
- Oral Hakan, Pappone Carlo, Chugh Aman, Good Eric, Bogun Frank, Pelosi Frank, Bates Eric R, Lehmann Michael H, Vicedomini Gabriele, Augello Giuseppe, Agricola Eustachio, Sala Simone, Santinelli Vincenzo, Morady Fred. Circumferential pulmonary-vein ablation for chronic atrial fibrillation. N. Engl. J. Med. 2006 Mar 02;354 (9):934–41. - PubMed
-
- Haïssaguerre Michel, Hocini Mélèze, Sanders Prashanthan, Sacher Frederic, Rotter Martin, Takahashi Yoshihide, Rostock Thomas, Hsu Li-Fern, Bordachar Pierre, Reuter Sylvain, Roudaut Raymond, Clémenty Jacques, Jaïs Pierre. Catheter ablation of long-lasting persistent atrial fibrillation: clinical outcome and mechanisms of subsequent arrhythmias. J. Cardiovasc. Electrophysiol. 2005 Nov;16 (11):1138–47. - PubMed
Publication types
LinkOut - more resources
Full Text Sources