

Under Pressure: Intraluminal Filling Pressures of Postpartum Hemorrhage Tamponade Balloons
- PMID: 28497006
- PMCID: PMC5423810
- DOI: 10.1055/s-0037-1602657
Under Pressure: Intraluminal Filling Pressures of Postpartum Hemorrhage Tamponade Balloons
Abstract
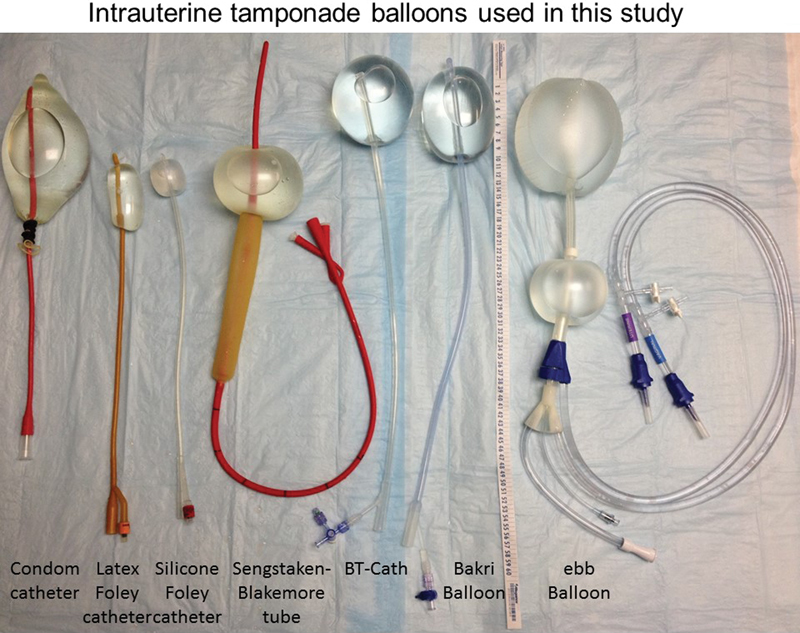
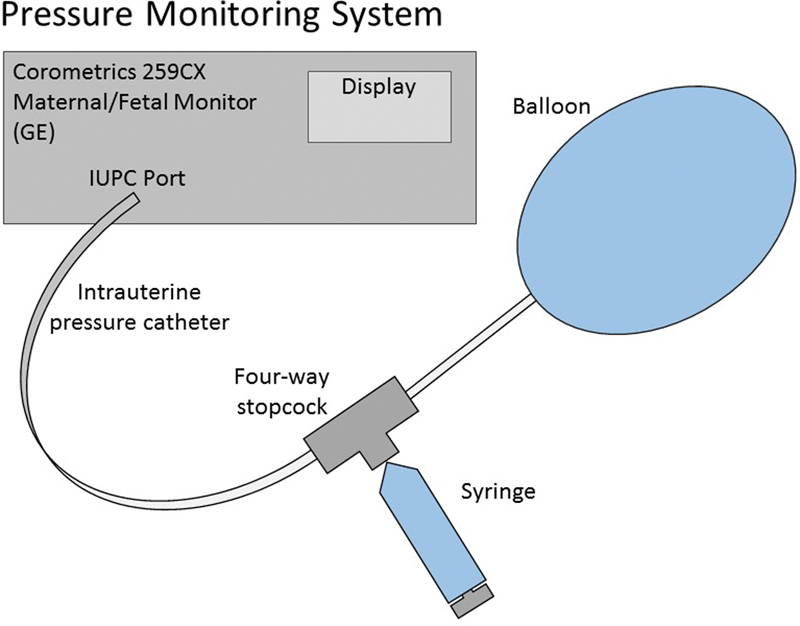
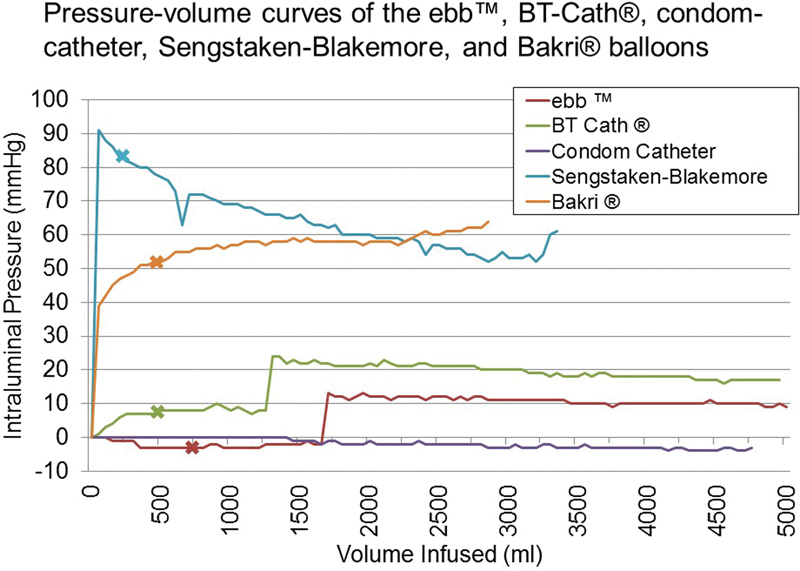
Objective Uterine tamponade by fluid-filled balloons is now an accepted method of controlling postpartum hemorrhage. Available tamponade balloons vary in design and material, which affects the filling attributes and volume at which they rupture. We aimed to characterize the filling capacity and pressure-volume relationship of various tamponade balloons. Study Design Balloons were filled with water ex vivo. Intraluminal pressure was measured incrementally (every 10 mL for the Foley balloons and every 50 mL for all other balloons). Balloons were filled until they ruptured or until 5,000 mL was reached. Results The Foley balloons had higher intraluminal pressures than the larger-volume balloons. The intraluminal pressure of the Sengstaken-Blakemore tube (gastric balloon) was initially high, but it decreased until shortly before rupture occurred. The Bakri intraluminal pressure steadily increased until rupture occurred at 2,850 mL. The condom catheter, BT-Cath, and ebb all had low intraluminal pressures. Both the BT-Cath and the ebb remained unruptured at 5,000 mL. Conclusion In the setting of acute hemorrhage, expeditious management is critical. Balloons that have a low intraluminal pressure-volume ratio may fill more rapidly, more easily, and to greater volumes. We found that the BT-Cath, the ebb, and the condom catheter all had low intraluminal pressures throughout filling.
Keywords: BT-Cath; Bakri balloon; ebb balloon; intraluminal pressure; postpartum hemorrhage; uterine balloon; uterine balloon tamponade; uterine tamponade; uterine tamponade balloon.
Conflict of interest statement
Figures

References
-
- Callaghan W M, Kuklina E V, Berg C J. Trends in postpartum hemorrhage: United States, 1994–2006. Am J Obstet Gynecol. 2010;202(04):3530–3.53E8. - PubMed
-
- Kramer M S, Berg C, Abenhaim H et al. Incidence, risk factors, and temporal trends in severe postpartum hemorrhage. Am J Obstet Gynecol. 2013;209(05):4490–4.49E9. - PubMed
-
- Division of Reproductive Health Centers for Disease Control and Prevention NC for CDP and HP. Pregnancy Mortality Surveillance System: Causes of Pregnancy-Related Death in the United States, 2006–2009 Pregnancy Mortal Surveill Syst 200958972–975.
-
- Clark S L, Belfort M A, Dildy G A, Herbst M A, Meyers J A, Hankins G D.Maternal death in the 21st century: causes, prevention, and relationship to cesarean delivery Am J Obstet Gynecol 200819901360–3.6E6., discussion 91–92, e7–e11 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources