

The waterfall effect in breast augmentation
- PMID: 28497023
- PMCID: PMC5409900
- DOI: 10.21037/gs.2016.10.01
The waterfall effect in breast augmentation
Abstract
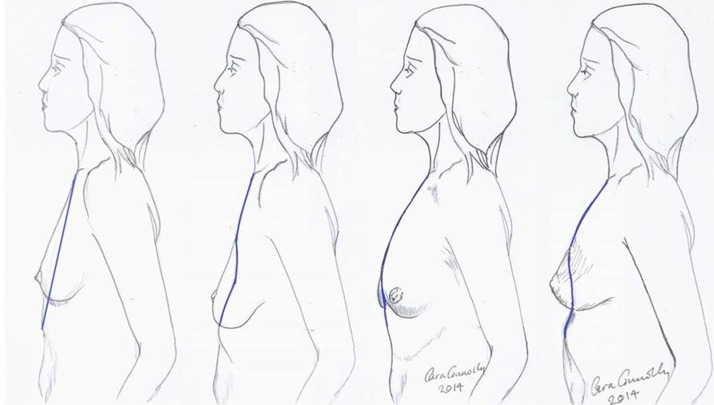
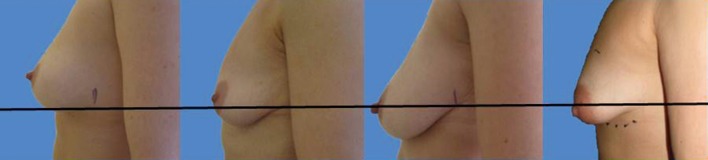
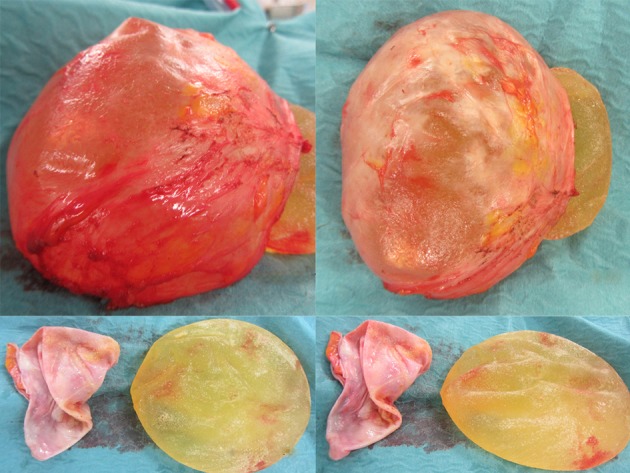
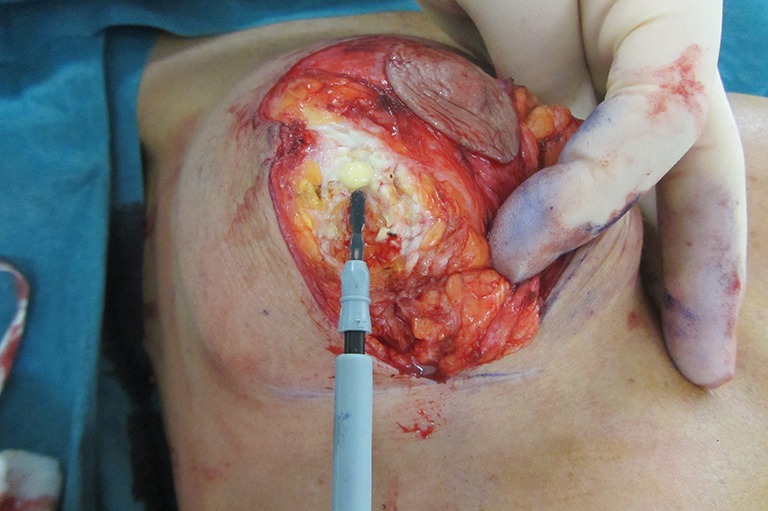
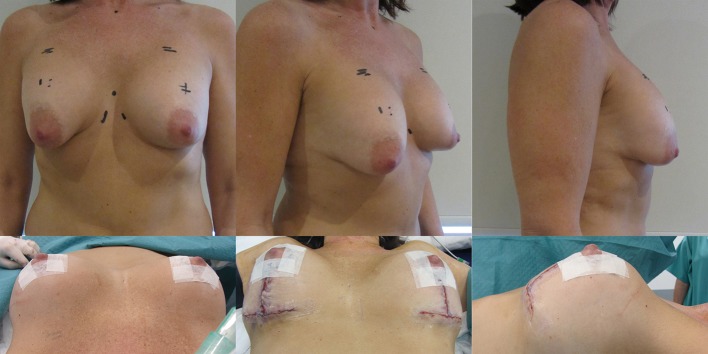
The 'waterfall effect' is a descriptive term to indicate a sliding ptosis of parenchymal breast tissue over a fixed or encapsulated implant. It occurs more frequently than surgeons anticipate and especially over the longer term after augmentation. Certain breast implants are more prone to contribute to this problem as are implants placed in submuscular pockets that ride high, especially in women with anatomical musculoskeletal variance or asymmetry. This article describes the aetiology of sliding ptosis in more detail, the relevant anatomy and the surgical correction. Understanding the problem enables the surgeon to plan the appropriate procedure and obtain proper informed consent. It is possible that a two stage procedure is necessary should the upper pole of breast require a debulk, either early (3 to 12 months) or later as the breast may slide with ageing of the tissues. The waterfall effect of breast parenchyma over implants is only apparent when the upper torso of the woman is undressed and she is in an erect posture. A significant number of women are happy with this situation and therefore no further action is required. Those that want an improved appearance in these circumstances can try autologous fat transfer to rebulk the surrounding tissues but generally the most likely solution involves a mastopexy with or without implant exchange. The results are highly rewarding but the scars are the legacy. Mastopexy augmentation is a difficult procedure and should only be performed by experienced surgeons. Many surgeons prefer a two stage approach with either an implant based augmentation first to limit scars and see if the patient is happy with the outcome or a first stage mastopexy to decide whether implants or fat graft are actually required as a secondary procedure.
Keywords: Breast mastopexy; breast implants; breast parenchyma; breast ptosis; pectoralis major muscle; polyurethane breast implants; silicone.
Conflict of interest statement
Conflicts of Interest: The author has no conflicts of interest to declare.
Figures















References
-
- McCulley S. How Many Women Have Breast Implants? Available online: http://www.stephenmcculley.co.uk/how-many-women-have-breast-implants/
-
- UK Progressive. Dear Mona, What Percentage Of Women Have Breast Implants? Available online: http://www.ukprogressive.co.uk/dear-mona-what-percentage-of-women-have-b...
-
- Center for Devices and Radiological Health U.S. Food and Drug Administration. FDA Update on the Safety of Silicone Gel-Filled Breast. Available online: http://www.fda.gov/downloads/MedicalDevices/ProductsandMedicalProcedures...
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources