

Performance of a capnodynamic method estimating effective pulmonary blood flow during transient and sustained hypercapnia
- PMID: 28497180
- PMCID: PMC5838142
- DOI: 10.1007/s10877-017-0021-3
Performance of a capnodynamic method estimating effective pulmonary blood flow during transient and sustained hypercapnia
Abstract
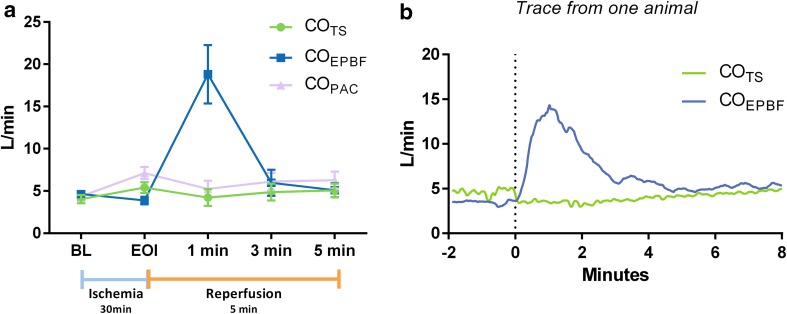
The capnodynamic method is a minimally invasive method continuously calculating effective pulmonary blood flow (COEPBF), equivalent to cardiac output when intra pulmonary shunt flow is low. The capnodynamic equation joined with a ventilator pattern containing cyclic reoccurring expiratory holds, provides breath to breath hemodynamic monitoring in the anesthetized patient. Its performance however, might be affected by changes in the mixed venous content of carbon dioxide (CvCO2). The aim of the current study was to evaluate COEPBF during rapid measurable changes in mixed venous carbon dioxide partial pressure (PvCO2) following ischemia-reperfusion and during sustained hypercapnia in a porcine model. Sixteen pigs were submitted to either ischemia-reperfusion (n = 8) after the release of an aortic balloon inflated during 30 min or to prolonged hypercapnia (n = 8) induced by adding an instrumental dead space. Reference cardiac output (CO) was measured by an ultrasonic flow probe placed around the pulmonary artery trunk (COTS). Hemodynamic measurements were obtained at baseline, end of ischemia and during the first 5 min of reperfusion as well as during prolonged hypercapnia at high and low CO states. Ischemia-reperfusion resulted in large changes in PvCO2, hemodynamics and lactate. Bias (limits of agreement) was 0.7 (-0.4 to 1.8) L/min with a mean error of 28% at baseline. COEPBF was impaired during reperfusion but agreement was restored within 5 min. During prolonged hypercapnia, agreement remained good during changes in CO. The mean polar angle was -4.19° (-8.8° to 0.42°). Capnodynamic COEPBF is affected but recovers rapidly after transient large changes in PvCO2 and preserves good agreement and trending ability during states of prolonged hypercapnia at different levels of CO.
Keywords: Animal model; Capnodynamic; Carbon dioxide; Cardiac output; Effective pulmonary blood flow; Intraoperative monitoring.
Conflict of interest statement
Conflict of interest
Magnus Hallbäck and Mats Wallin are employed at Maquet Critical Care AB (MCC). Fernando Suarez Sipmann performs consultant activities for MCC. Håkan Björne and Caroline Hällsjö Sander has received grants for research from MCC. Thorir Sigmundsson, Tomas Öhman, Eider Redondo, Anders Oldner declare no conflict of interest.
Ethical approval
The study was approved by the Uppsala animal research ethical committee (nr. C 47/15) and performed at the Hedenstierna laboratory in Uppsala University, Sweden. All applicable international, national, and/or institutional guidelines for the care and use of animals were followed.
Figures


References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
