

The role of high airway pressure and dynamic strain on ventilator-induced lung injury in a heterogeneous acute lung injury model
- PMID: 28497420
- PMCID: PMC5427060
- DOI: 10.1186/s40635-017-0138-1
The role of high airway pressure and dynamic strain on ventilator-induced lung injury in a heterogeneous acute lung injury model
Abstract
Background: Acute respiratory distress syndrome causes a heterogeneous lung injury with normal and acutely injured lung tissue in the same lung. Improperly adjusted mechanical ventilation can exacerbate ARDS causing a secondary ventilator-induced lung injury (VILI). We hypothesized that a peak airway pressure of 40 cmH2O (static strain) alone would not cause additional injury in either the normal or acutely injured lung tissue unless combined with high tidal volume (dynamic strain).
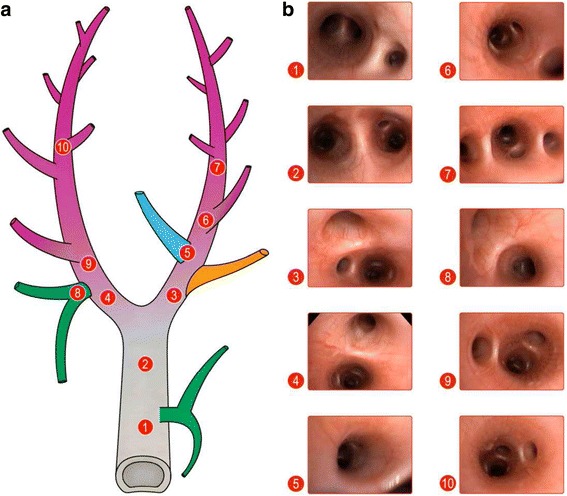
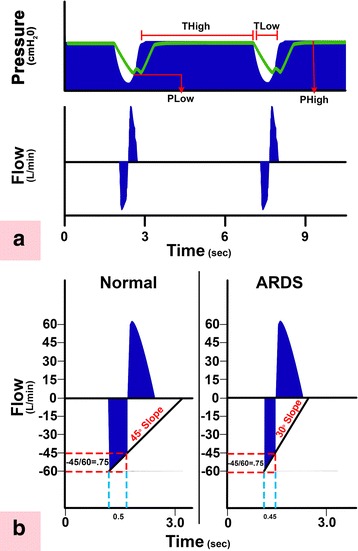
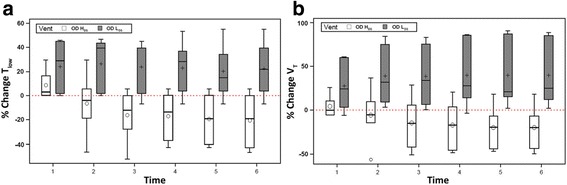
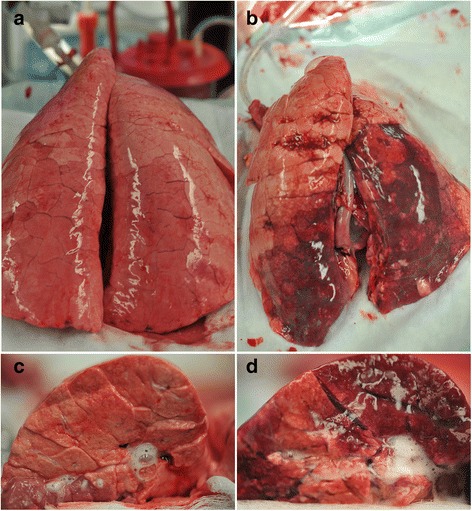
Methods: Pigs were anesthetized, and heterogeneous acute lung injury (ALI) was created by Tween instillation via a bronchoscope to both diaphragmatic lung lobes. Tissue in all other lobes was normal. Airway pressure release ventilation was used to precisely regulate time and pressure at both inspiration and expiration. Animals were separated into two groups: (1) over-distension + high dynamic strain (OD + HDS, n = 6) and (2) over-distension + low dynamic strain (OD + LDS, n = 6). OD was caused by setting the inspiratory pressure at 40 cmH2O and dynamic strain was modified by changing the expiratory duration, which varied the tidal volume. Animals were ventilated for 6 h recording hemodynamics, lung function, and inflammatory mediators followed by an extensive necropsy.
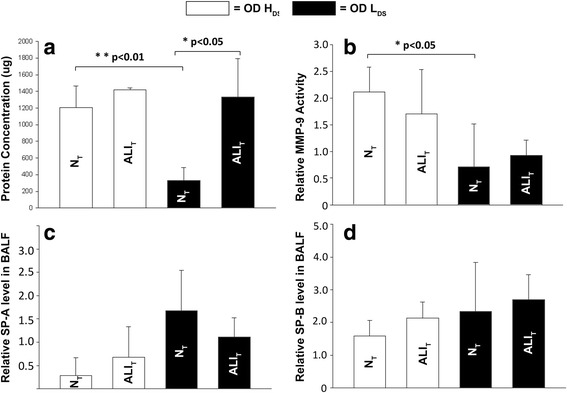
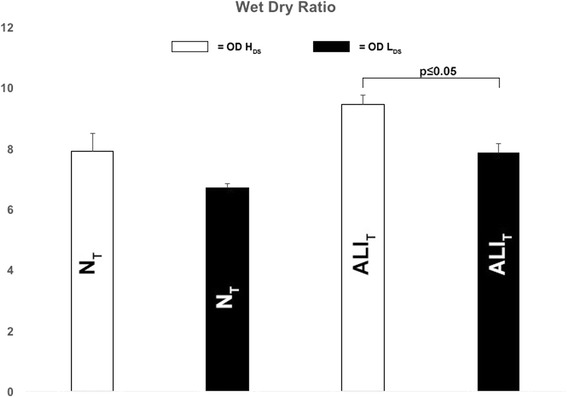
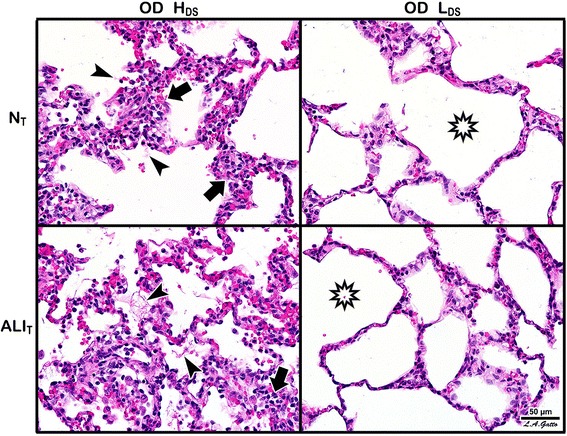
Results: In normal tissue (NT), OD + LDS caused minimal histologic damage and a significant reduction in BALF total protein (p < 0.05) and MMP-9 activity (p < 0.05), as compared with OD + HDS. In acutely injured tissue (ALIT), OD + LDS resulted in reduced histologic injury and pulmonary edema (p < 0.05), as compared with OD + HDS.
Conclusions: Both NT and ALIT are resistant to VILI caused by OD alone, but when combined with a HDS, significant tissue injury develops.
Keywords: Acute lung injury; Acute respiratory distress syndrome (ARDS); Alveolar collapse and reexpansion; Alveolar over-distension; Atelectasis; Dynamic strain; Heterogeneous lung; Heterogeneous lung inflation; Over-distension; Static strain; Strain; Stress; Ventilator-induced lung injury (VILI).
Figures
Similar articles
-
Protective ventilation in a pig model of acute lung injury: timing is as important as pressure.J Appl Physiol (1985). 2022 Nov 1;133(5):1093-1105. doi: 10.1152/japplphysiol.00312.2022. Epub 2022 Sep 22. J Appl Physiol (1985). 2022. PMID: 36135956 Free PMC article.
-
Altered alveolar mechanics in the acutely injured lung.Crit Care Med. 2001 May;29(5):1049-55. doi: 10.1097/00003246-200105000-00036. Crit Care Med. 2001. PMID: 11383531
-
Alveolar inflation during generation of a quasi-static pressure/volume curve in the acutely injured lung.Crit Care Med. 2003 Apr;31(4):1126-33. doi: 10.1097/01.CCM.0000059997.90832.29. Crit Care Med. 2003. PMID: 12682483
-
First Stabilize and then Gradually Recruit: A Paradigm Shift in Protective Mechanical Ventilation for Acute Lung Injury.J Clin Med. 2023 Jul 12;12(14):4633. doi: 10.3390/jcm12144633. J Clin Med. 2023. PMID: 37510748 Free PMC article. Review.
-
Prevention and treatment of acute lung injury with time-controlled adaptive ventilation: physiologically informed modification of airway pressure release ventilation.Ann Intensive Care. 2020 Jan 6;10(1):3. doi: 10.1186/s13613-019-0619-3. Ann Intensive Care. 2020. PMID: 31907704 Free PMC article. Review.
Cited by
-
A Physiologically Informed Strategy to Effectively Open, Stabilize, and Protect the Acutely Injured Lung.Front Physiol. 2020 Mar 19;11:227. doi: 10.3389/fphys.2020.00227. eCollection 2020. Front Physiol. 2020. PMID: 32265734 Free PMC article. Review.
-
Closing, opening and reopening: the difficult coexistence.J Thorac Dis. 2017 Jul;9(7):1808-1810. doi: 10.21037/jtd.2017.06.93. J Thorac Dis. 2017. PMID: 28839970 Free PMC article. No abstract available.
-
Mechanical Power and Ventilator-induced Lung Injury: What Does Physics Have to Say?Am J Respir Crit Care Med. 2024 Apr 1;209(7):787-788. doi: 10.1164/rccm.202307-1292VP. Am J Respir Crit Care Med. 2024. PMID: 37729623 Free PMC article. No abstract available.
-
Acute lung injury: how to stabilize a broken lung.Crit Care. 2018 May 24;22(1):136. doi: 10.1186/s13054-018-2051-8. Crit Care. 2018. PMID: 29793554 Free PMC article.
-
Protective ventilation in a pig model of acute lung injury: timing is as important as pressure.J Appl Physiol (1985). 2022 Nov 1;133(5):1093-1105. doi: 10.1152/japplphysiol.00312.2022. Epub 2022 Sep 22. J Appl Physiol (1985). 2022. PMID: 36135956 Free PMC article.
References
-
- Guerin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, Mercier E, Badet M, Mercat A, Baudin O, Clavel M, Chatellier D, Jaber S, Rosselli S, Mancebo J, Sirodot M, Hilbert G, Bengler C, Richecoeur J, Gainnier M, Bayle F, Bourdin G, Leray V, Girard R, Baboi L, Ayzac L, Group PS Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368:2159–2168. doi: 10.1056/NEJMoa1214103. - DOI - PubMed
-
- Nieman GF, Gatto LA, Habashi NM. Impact of mechanical ventilation on the pathophysiology of progressive acute lung injury. J Appl Physiol. 2015;119:1245–1261. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
