

The Impact of Preexposure Prophylaxis Among Men Who Have Sex With Men: An Individual-Based Model
- PMID: 28498144
- PMCID: PMC5488295
- DOI: 10.1097/QAI.0000000000001354
The Impact of Preexposure Prophylaxis Among Men Who Have Sex With Men: An Individual-Based Model
Abstract
Objectives: Preexposure prophylaxis (PrEP) is recommended for preventing HIV infection among individuals at high risk, including men who have sex with men (MSM). Although its individual-level efficacy is proven, questions remain regarding population-level impact of PrEP implementation.
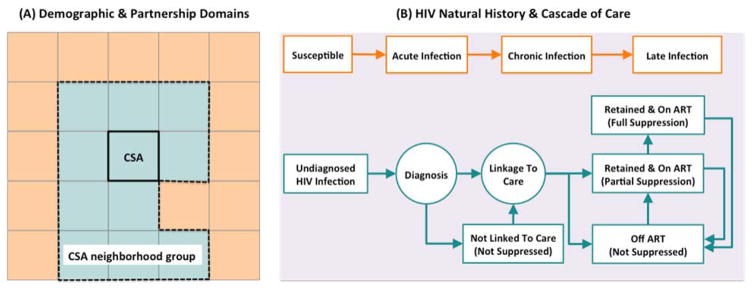
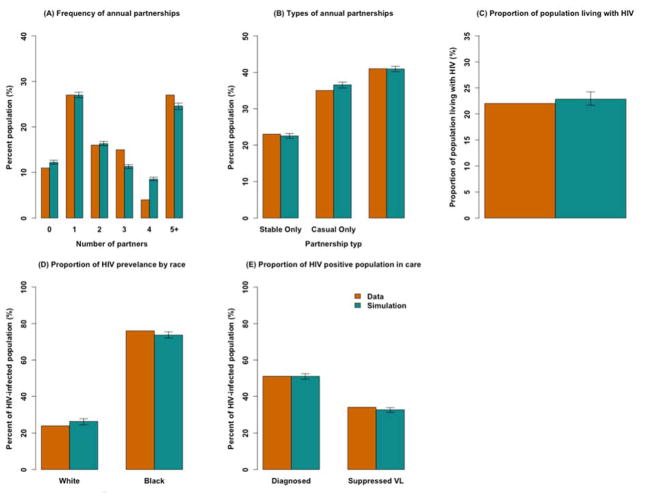
Design: We developed an agent-based simulation of HIV transmission among MSM, accounting for demographics, sexual contact network, HIV disease stage, and use of antiretroviral therapy. We use this framework to compare PrEP delivery strategies in terms of impact on HIV incidence and prevalence.
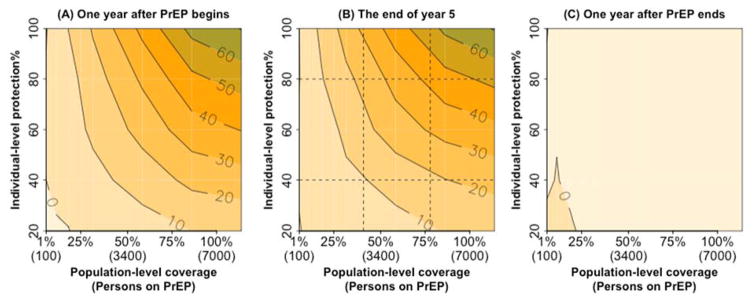
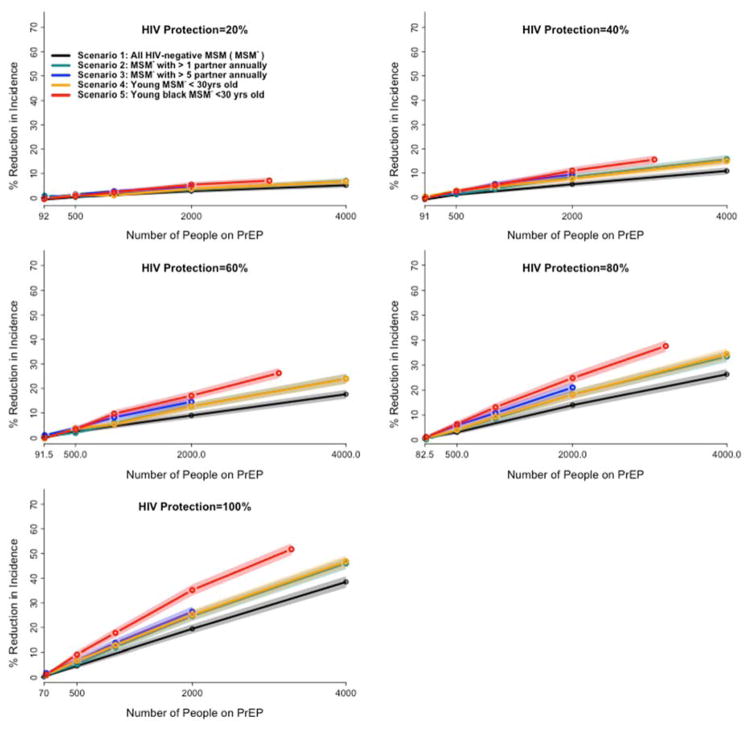
Results: The projected reduction in HIV incidence achievable with PrEP reflects both population-level coverage and individual-level adherence (as a proportion of days protected against HIV transmission). For example, provision of PrEP to 40% of HIV-negative MSM reporting more than one sexual partner in the last 12 months, taken with sufficient adherence to provide protection on 40% of days, can reduce HIV incidence by 9.5% (95% uncertainty range: 8%-11%) within 5 years. However, if this could be increased to 80% coverage on 80% of days (eg, through mass campaigns with a long-acting injectable formulation), a 43% (42%-44%) reduction in HIV incidence could be achieved. Delivering PrEP to MSM at high risk for HIV acquisition can augment population-level impact up to 1.8-fold.
Conclusions: If highly ambitious targets for coverage and adherence can be achieved, PrEP can substantially reduce HIV incidence in the short-term. Although the reduction in HIV incidence largely reflects the proportion of person-years protected, the efficiency of PrEP delivery can be enhanced by targeting high-risk populations.
Figures
References
-
- Thigpen MC, Kebaabetswe PM, Paxton LA, Smith DK, Rose CE, Segolodi TM, et al. Antiretroviral preexposure prophylaxis for heterosexual HIV transmission in Botswana. N Engl J Med. 2012;367:423–34. - PubMed
-
- U.S. Food and Drug Administration. FDA Approves First Medication to Reduce HIV Risk. Consum Updat. 2016
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
