

High Frequency of Neuroimaging Abnormalities Among Pediatric Patients With Sepsis Who Undergo Neuroimaging
- PMID: 28498230
- PMCID: PMC5503765
- DOI: 10.1097/PCC.0000000000001173
High Frequency of Neuroimaging Abnormalities Among Pediatric Patients With Sepsis Who Undergo Neuroimaging
Abstract
Objectives: This study was intended to describe and correlate the neuroimaging findings in pediatric patients after sepsis.
Design: Retrospective chart review.
Setting: Single tertiary care PICU.
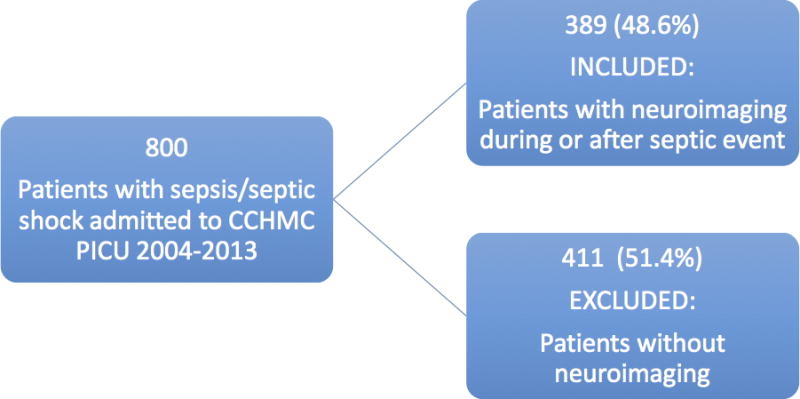
Patients: Patients admitted to Cincinnati Children's Hospital Medical Center with a discharge diagnosis of sepsis or septic shock between 2004 and 2013 were crossmatched with patients who underwent neuroimaging during the same time period.
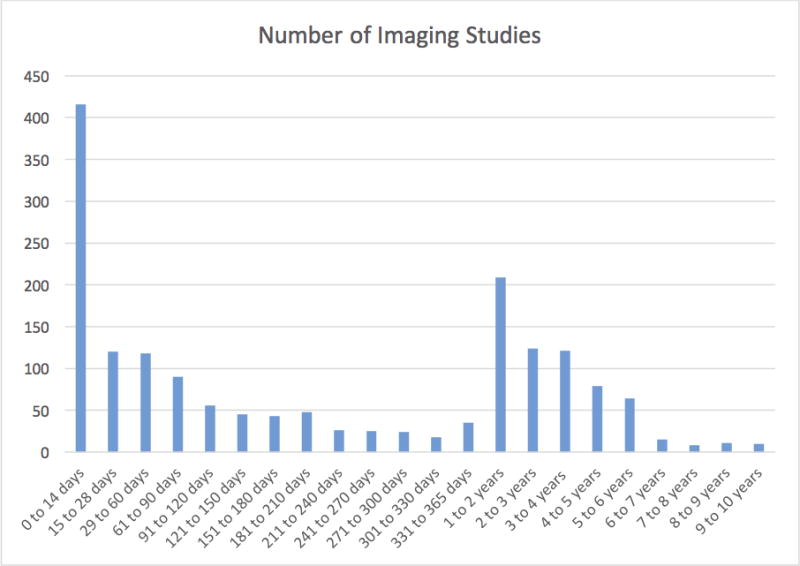
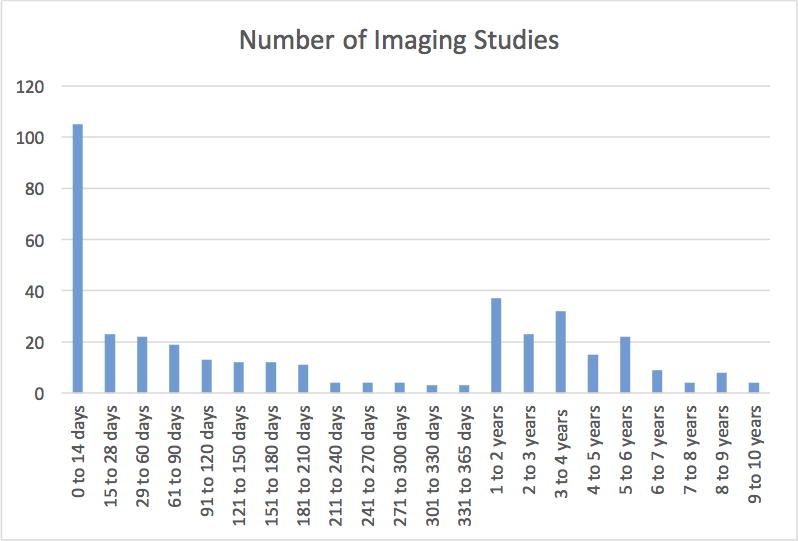
Interventions: All neuroimaging studies that occurred during or subsequent to a septic event were reviewed, and all new imaging findings were recorded and classified. As many patients experienced multiple septic events and/or had multiple neuroimaging studies after sepsis, our statistical analysis utilized the most recent or "final" imaging study available for each patient so that only brain imaging findings that persisted were included.
Measurements and main results: A total of 389 children with sepsis and 1,705 concurrent or subsequent neuroimaging studies were included in the study. Median age at first septic event was 3.4 years (interquartile range, 0.7-11.5). Median time from first sepsis event to final neuroimaging was 157 days (interquartile range, 10-1,054). The most common indications for final imaging were follow-up (21%), altered mental status (18%), and fever/concern for infection (15%). Sixty-three percentage (n = 243) of final imaging studies demonstrated abnormal findings, the most common of which were volume loss (39%) and MRI signal and/or CT attenuation abnormalities (21%). On multivariable logistic regression, highest Pediatric Risk of Mortality score and presence of oncologic diagnosis/organ transplantation were independently associated with any abnormal final neuroimaging study findings (odds ratio, 1.032; p = 0.048 and odds ratio, 1.632; p = 0.041), although early timing of neuroimaging demonstrated a negative association (odds ratio, 0.606; p = 0.039). The most common abnormal finding of volume loss was independently associated with highest Pediatric Risk of Mortality score (odds ratio, 1.037; p = 0.016) and oncologic diagnosis/organ transplantation (odds ratio, 2.207; p = 0.001) and was negatively associated with early timing of neuroimaging (odds ratio, 0.575; p = 0.037).
Conclusions: The majority of pediatric patients with sepsis and concurrent or subsequent neuroimaging have abnormal neuroimaging findings. The implications of this high incidence for long-term neurologic outcomes and follow-up require further exploration.
Conflict of interest statement
Conflicts of interest: none declared
Copyright form disclosure:
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003;31(4):1250–6. - PubMed
-
- Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302(21):2323–9. - PubMed
-
- Sprung CL, Peduzzi PN, Shatney CH, Schein RM, Wilson MF, Sheagren JN, et al. Impact of encephalopathy on mortality in the sepsis syndrome. The Veterans Administration Systemic Sepsis Cooperative Study Group. Crit Care Med. 1990;18(8):801–6. - PubMed
-
- Gofton TE, Young GB. Sepsis-associated encephalopathy. Nat Rev Neurol. 2012;8(10):557–66. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
