

A third generation vaccine for human visceral leishmaniasis and post kala azar dermal leishmaniasis: First-in-human trial of ChAd63-KH
- PMID: 28498840
- PMCID: PMC5443534
- DOI: 10.1371/journal.pntd.0005527
A third generation vaccine for human visceral leishmaniasis and post kala azar dermal leishmaniasis: First-in-human trial of ChAd63-KH
Abstract
Background: Visceral leishmaniasis (VL or kala azar) is the most serious form of human leishmaniasis, responsible for over 20,000 deaths annually, and post kala azar dermal leishmaniasis (PKDL) is a stigmatizing skin condition that often occurs in patients after successful treatment for VL. Lack of effective or appropriately targeted cell mediated immunity, including CD8+ T cell responses, underlies the progression of VL and progression to PKDL, and can limit the therapeutic efficacy of anti-leishmanial drugs. Hence, in addition to the need for prophylactic vaccines against leishmaniasis, the development of therapeutic vaccines for use alone or in combined immuno-chemotherapy has been identified as an unmet clinical need. Here, we report the first clinical trial of a third-generation leishmaniasis vaccine, developed intentionally to induce Leishmania-specific CD8+ T cells.
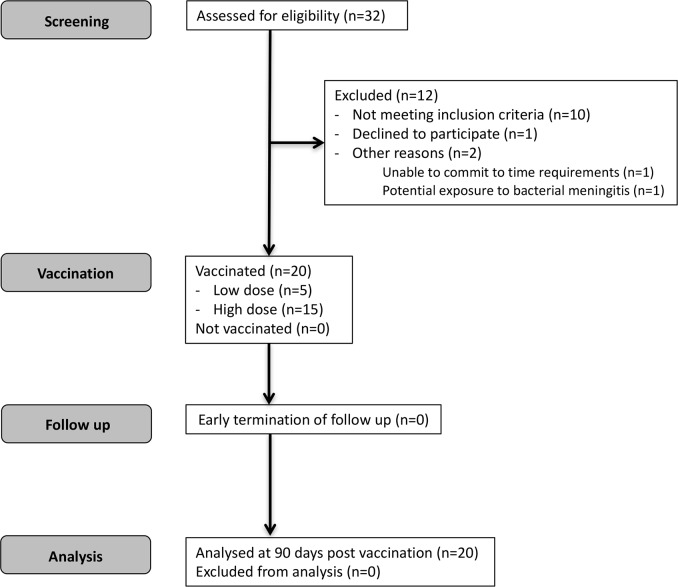
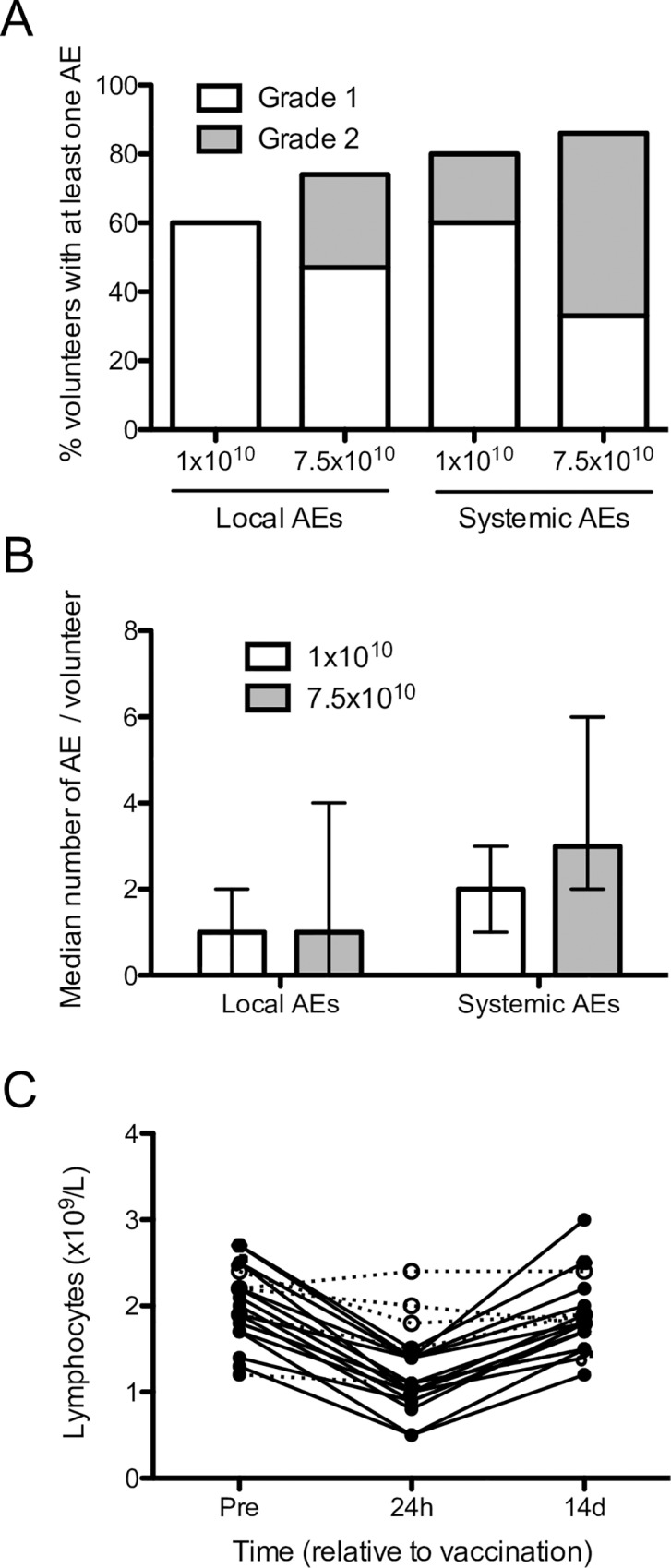
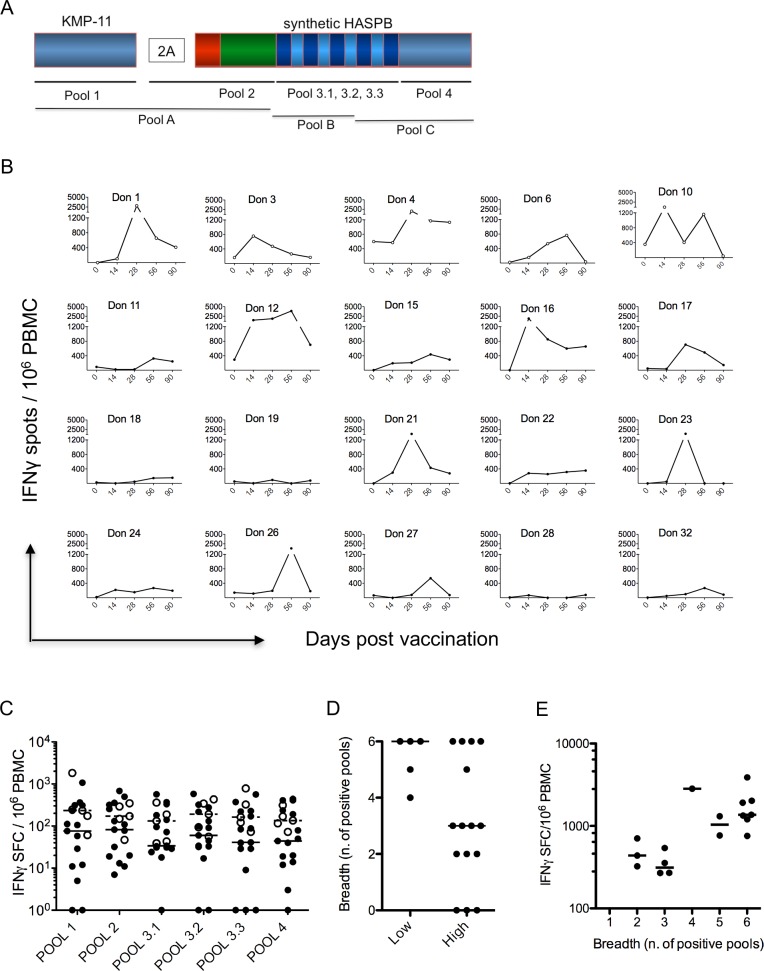
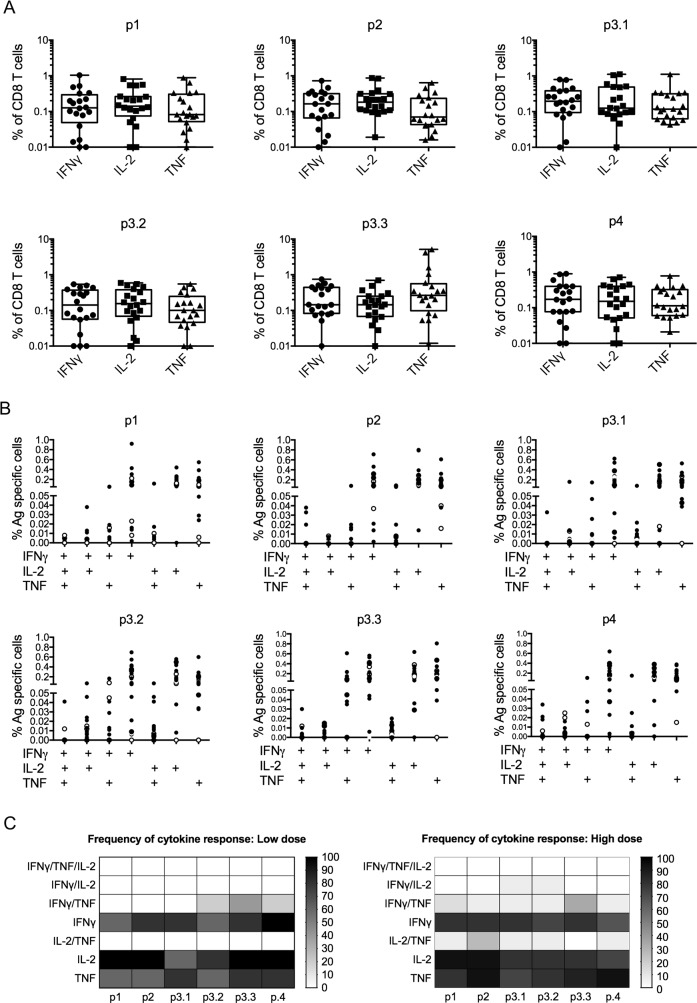
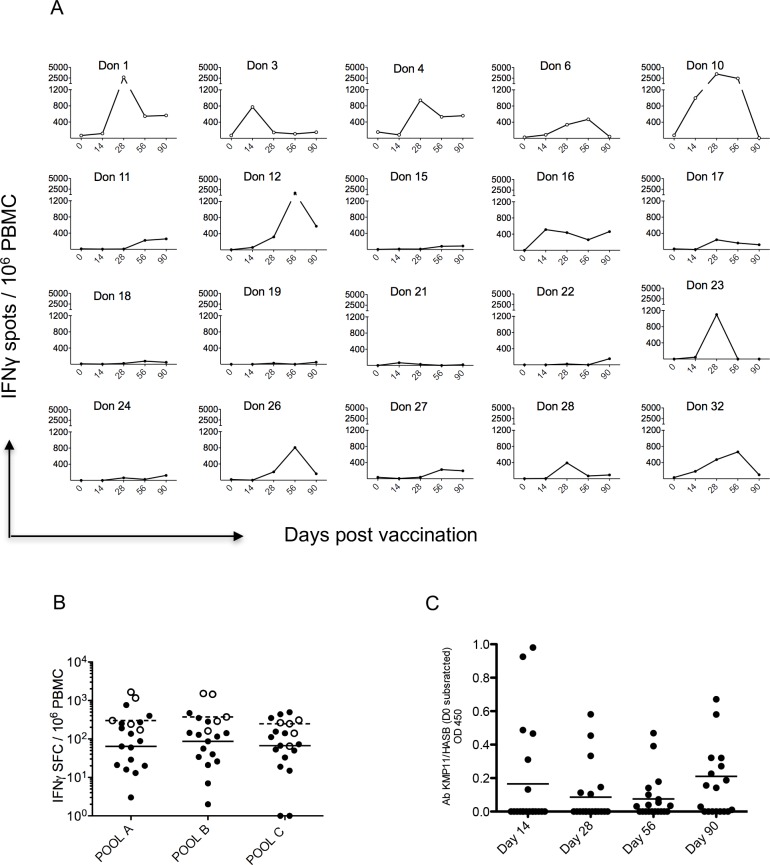
Methods: We conducted a first-in-human dose escalation Phase I trial in 20 healthy volunteers to assess the safety, tolerability and immunogenicity of a prime-only adenoviral vaccine for human VL and PKDL. ChAd63-KH is a replication defective simian adenovirus expressing a novel synthetic gene (KH) encoding two Leishmania proteins KMP-11 and HASPB. Uniquely, the latter was engineered to reflect repeat domain polymorphisms and arrangements identified from clinical isolates. We monitored innate immune responses by whole blood RNA-Seq and antigen specific CD8+ T cell responses by IFNγ ELISPOT and intracellular flow cytometry.
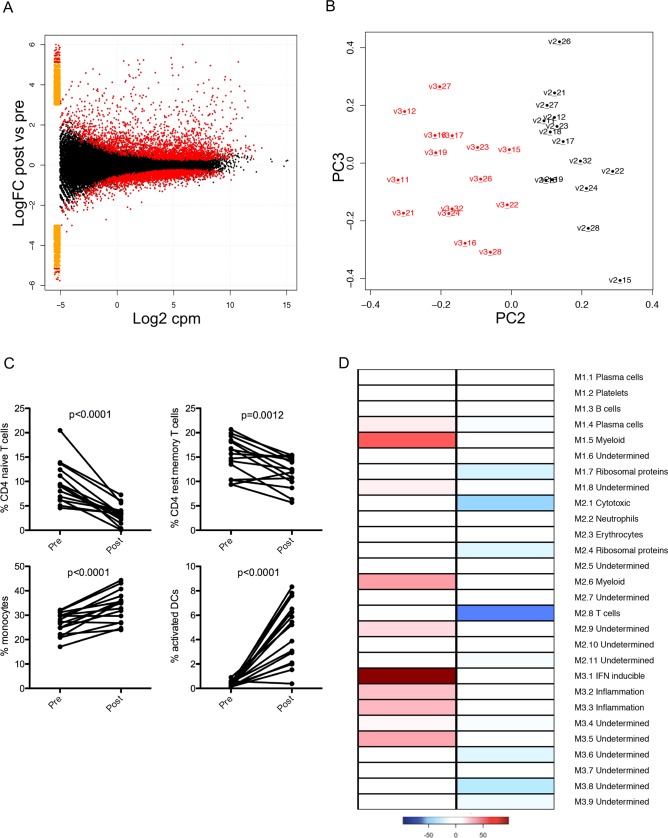
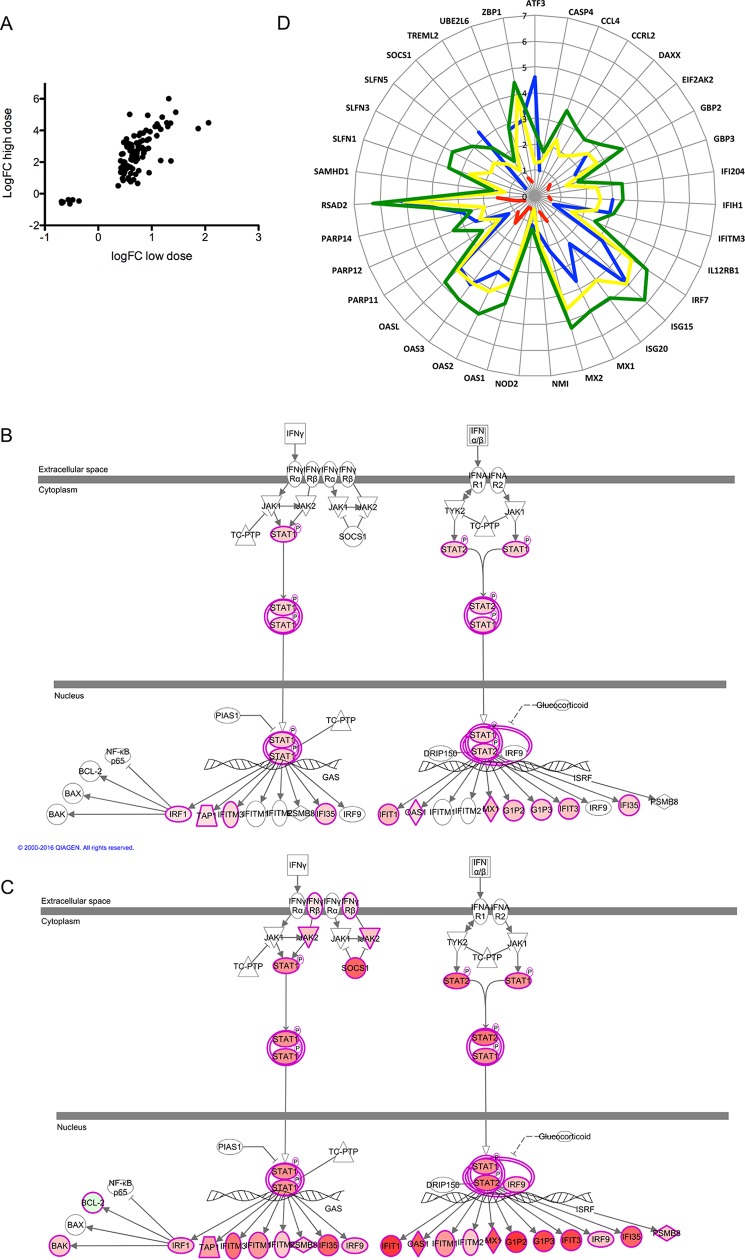
Findings: ChAd63-KH was safe at intramuscular doses of 1x1010 and 7.5x1010 vp. Whole blood transcriptomic profiling indicated that ChAd63-KH induced innate immune responses characterized by an interferon signature and the presence of activated dendritic cells. Broad and quantitatively robust CD8+ T cell responses were induced by vaccination in 100% (20/20) of vaccinated subjects.
Conclusion: The results of this study support the further development of ChAd63-KH as a novel third generation vaccine for VL and PKDL.
Trial registration: This clinical trial (LEISH1) was registered at EudraCT (2012-005596-14) and ISRCTN (07766359).
Conflict of interest statement
The synthetic gene KH is subject to a patent (no 10719953.1) awarded to the University of York and the University of Edinburgh (inventors PMK, TA, CL and DFS). SDM, SC and LS are employees of ReiThera SRl. RC was an employee of Keires Ag.
Figures
References
-
- Alvar J, Velez ID, Bern C, Herrero M, Desjeux P, Cano J, et al. Leishmaniasis worldwide and global estimates of its incidence. PloS one. 2012;7(5):e35671 Epub 2012/06/14. PubMed Central PMCID: PMC3365071. doi: 10.1371/journal.pone.0035671 - DOI - PMC - PubMed
-
- Alvar J, Croft SL, Kaye P, Khamesipour A, Sundar S, Reed SG. Case study for a vaccine against leishmaniasis. Vaccine. 2013;31 Suppl 2:B244–9. Epub 2013/04/26. - PubMed
-
- Evans KJ, Kedzierski L. Development of Vaccines against Visceral Leishmaniasis. Journal of tropical medicine. 2012;2012:892817 Epub 2011/09/14. PubMed Central PMCID: PMC3170777. doi: 10.1155/2012/892817 - DOI - PMC - PubMed
-
- Kaye PM, Aebischer T. Visceral leishmaniasis: immunology and prospects for a vaccine. Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases. 2011;17(10):1462–70. Epub 2011/08/20. - PubMed
-
- Convit J, Ulrich M, Zerpa O, Borges R, Aranzazu N, Valera M, et al. Immunotherapy of american cutaneous leishmaniasis in Venezuela during the period 1990–99. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2003;97(4):469–72. Epub 2004/07/21. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
