

Patterns of intravenous fluid resuscitation use in adult intensive care patients between 2007 and 2014: An international cross-sectional study
- PMID: 28498856
- PMCID: PMC5428917
- DOI: 10.1371/journal.pone.0176292
Patterns of intravenous fluid resuscitation use in adult intensive care patients between 2007 and 2014: An international cross-sectional study
Abstract
Background: In 2007, the Saline versus Albumin Fluid Evaluation-Translation of Research Into Practice Study (SAFE-TRIPS) reported that 0.9% sodium chloride (saline) and hydroxyethyl starch (HES) were the most commonly used resuscitation fluids in intensive care unit (ICU) patients. Evidence has emerged since 2007 that these fluids are associated with adverse patient-centred outcomes. Based on the published evidence since 2007, we sought to determine the current type of fluid resuscitation used in clinical practice and the predictors of fluid choice and determine whether these have changed between 2007 and 2014.
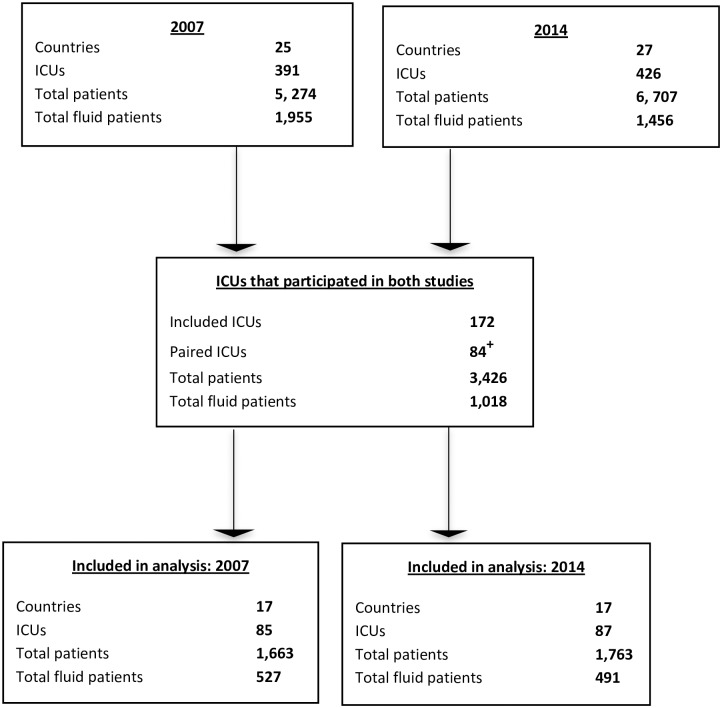
Methods: In 2014, an international, cross-sectional study was conducted (Fluid-TRIPS) to document current patterns of intravenous resuscitation fluid use and determine factors associated with fluid choice. We examined univariate and multivariate associations between patients and prescriber characteristics, geographical region and fluid type. Additionally, we report secular trends of resuscitation fluid use in a cohort of ICUs that participated in both the 2007 and 2014 studies. Regression analysis were conducted to determine changes in the administration of crystalloid or colloid between 2007 and 2014.
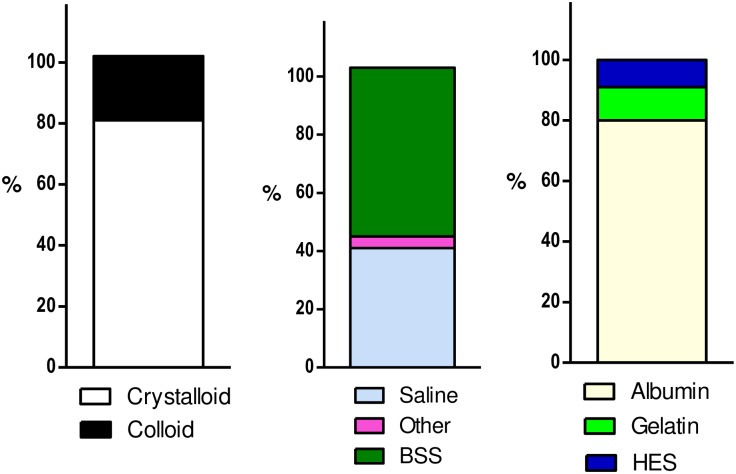
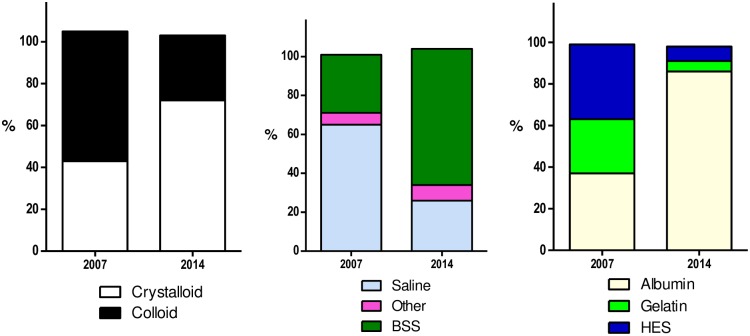
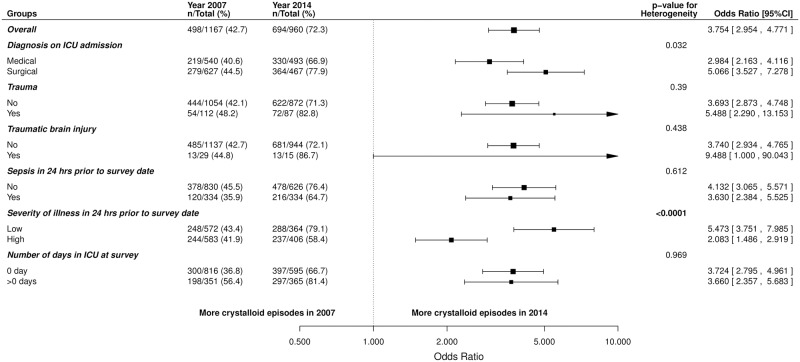
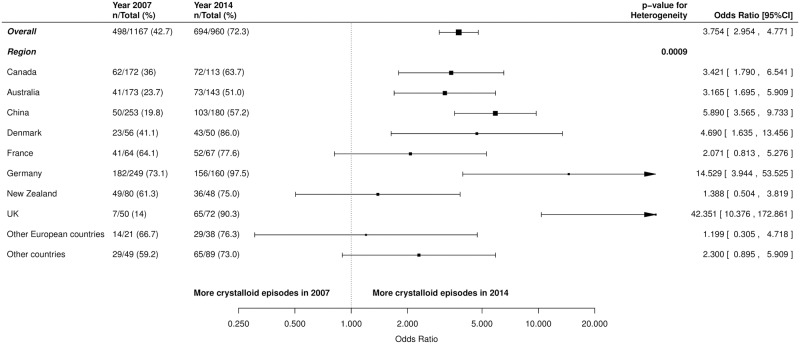
Findings: In 2014, a total of 426 ICUs in 27 countries participated. Over the 24 hour study day, 1456/6707 (21.7%) patients received resuscitation fluid during 2716 resuscitation episodes. Crystalloids were administered to 1227/1456 (84.3%) patients during 2208/2716 (81.3%) episodes and colloids to 394/1456 (27.1%) patients during 581/2716 (21.4%) episodes. In multivariate analyses, practice significantly varied between geographical regions. Additionally, patients with a traumatic brain injury were less likely to receive colloid when compared to patients with no trauma (adjusted OR 0.24; 95% CI 0.1 to 0.62; p = 0.003). Patients in the ICU for one or more days where more likely to receive colloid compared to patients in the ICU on their admission date (adjusted OR 1.75; 95% CI 1.27 to 2.41; p = <0.001). For secular trends in fluid resuscitation, 84 ICUs in 17 countries contributed data. In 2007, 527/1663 (31.7%) patients received fluid resuscitation during 1167 episodes compared to 491/1763 (27.9%) patients during 960 episodes in 2014. The use of crystalloids increased from 498/1167 (42.7%) in 2007 to 694/960 (72.3%) in 2014 (odds ratio (OR) 3.75, 95% confidence interval (CI) 2.95 to 4.77; p = <0.001), primarily due to a significant increase in the use of buffered salt solutions. The use of colloids decreased from 724/1167 (62.0%) in 2007 to 297/960 (30.9%) in 2014 (OR 0.29, 95% CI 0.19 to 0.43; p = <0.001), primarily due to a decrease in the use of HES, but an overall increase in the use of albumin.
Conclusions: Clinical practices of intravenous fluid resuscitation have changed between 2007 and 2014. Geographical location remains a strong predictor of the type of fluid administered for fluid resuscitation. Overall, there is a preferential use of crystalloids, specifically buffered salt solutions, over colloids. There is now an imperative to conduct a trial determining the safety and efficacy of these fluids on patient-centred outcomes.
Trial registration: Clinicaltrials.gov: Fluid-Translation of research into practice study (Fluid-TRIPS) NCT02002013.
Conflict of interest statement
Figures
References
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
