

The management of menopause in women with a history of endometriosis: a systematic review
- PMID: 28498913
- PMCID: PMC5850813
- DOI: 10.1093/humupd/dmx011
The management of menopause in women with a history of endometriosis: a systematic review
Abstract
Background: Endometriosis is typically regarded as a premenopausal disease, resolving after natural or iatrogenic menopause due to declining oestrogen levels. Nonetheless, case reports over the years have highlighted the incidence of recurrent postmenopausal endometriosis. It is now clear that both recurrence and malignant transformation of endometriotic foci can occur in the postmenopausal period. Postmenopausal women are commonly treated with hormone replacement therapy (HRT) to treat climacteric symptoms and prevent bone loss; however, HRT may reactivate endometriosis and stimulate malignant transformation in women with a history of endometriosis. Given the uncertain risks of initiating HRT, it is difficult to determine the best menopausal management for this group of women.
Objective and rational: The aim of this study was to systematically review the existing literature on management of menopausal symptoms in women with a history of endometriosis. We also aimed to evaluate the published literature on the risks associated with HRT in these women, and details regarding optimal formulations and timing (i.e. initiation and duration) of HRT.
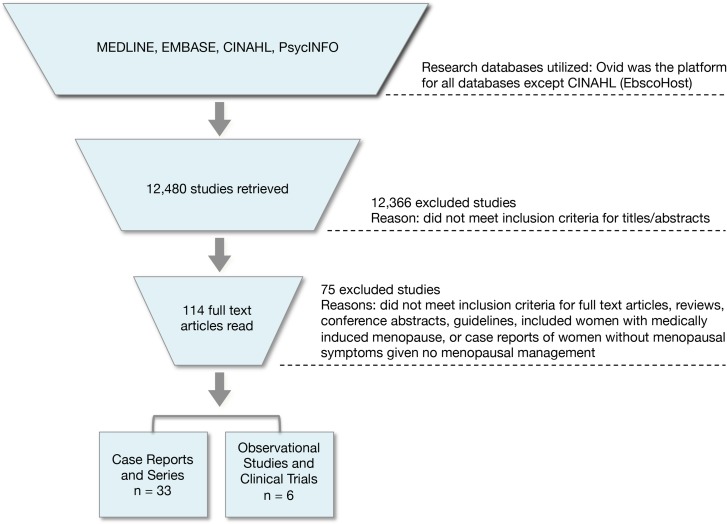
Search methods: Four electronic databases (MEDLINE via OVID, Embase via OVID, PsycINFO via OVID and CINAHL via EbscoHost) were searched from database inception until June 2016, using a combination of relevant controlled vocabulary terms and free-text terms related to 'menopause' and 'endometriosis'. Inclusion criteria were: menopausal women with a history of endometriosis and menopausal treatment including HRT or other preparations. Case reports/series, observational studies and clinical trials were included. Narrative review articles, organizational guidelines and conference abstracts were excluded, as were studies that did not report on any form of menopausal management. Articles were assessed for risk of bias and quality using GRADE criteria.
Outcomes: We present a synthesis of the existing case reports of endometriosis recurrence or malignant transformation in women undergoing treatment for menopausal symptoms. We highlight common presenting symptoms, potential risk factors and outcomes amongst the studies. Sparse high-quality evidence was identified, with few observational studies and only two randomized controlled trials. Given this paucity of data, no definitive conclusions can be drawn concerning risk.
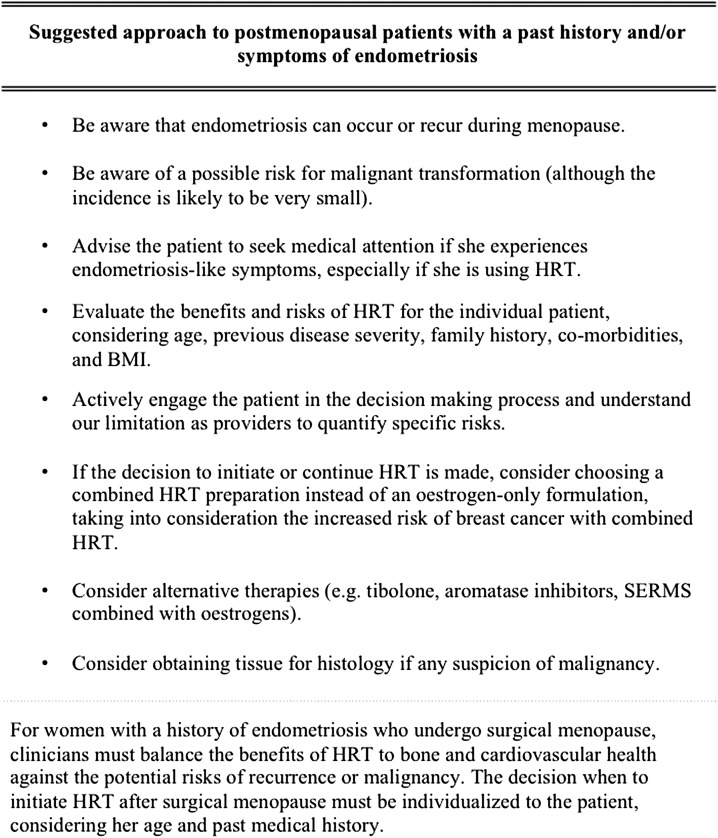
Wider implications: Due to the lack of high-quality studies, it remains unclear how to advise women with a history of endometriosis regarding the management of menopausal symptoms. The absolute risk of disease recurrence and malignant transformation cannot be quantified, and the impact of HRT use on these outcomes is not known. Multicentre randomized trials or large observational studies are urgently needed to inform clinicians and patients alike.
Keywords: HRT; combined HRT; endometriosis; malignant transformation; menopause; recurrence; tibolone; unopposed oestrogen.
© The Author 2017. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology.
Figures
References
-
- Abu MA, Sinha P, Totoe L, McCune G. Endometrial cancer thirteen years after total abdominal hysterectomy and bilateral salpingo-oophorectomy and hormone replacement therapy: a case report. Eur J Gynaecol Oncol 1997;18:482–483. - PubMed
-
- Ahn SH, Singh V, Tayade C. Biomarkers in endometriosis: challenges and opportunities. Fertil Steril 2017;107:523–532. - PubMed
-
- Al Kadri H, Hassan S, Al-Fozan HM, Hajeer A. Hormone therapy for endometriosis and surgical menopause. Cochrane Database Syst Rev 2009;Cd005997 doi: 10.1002/14651858.CD005997.pub2. - DOI - PubMed
-
- Al-Talib A, Gilbert L, Arseneau J. Endometrioid adenocarcinoma 13 years after total abdominal hysterectomy and bilateral salpingo-oophorectomy. Saudi Med J 2008;29:1044–1047. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
