

Clinical classification in low back pain: best-evidence diagnostic rules based on systematic reviews
- PMID: 28499364
- PMCID: PMC5429540
- DOI: 10.1186/s12891-017-1549-6
Clinical classification in low back pain: best-evidence diagnostic rules based on systematic reviews
Abstract
Background: Clinical examination findings are used in primary care to give an initial diagnosis to patients with low back pain and related leg symptoms. The purpose of this study was to develop best evidence Clinical Diagnostic Rules (CDR] for the identification of the most common patho-anatomical disorders in the lumbar spine; i.e. intervertebral discs, sacroiliac joints, facet joints, bone, muscles, nerve roots, muscles, peripheral nerve tissue, and central nervous system sensitization.
Methods: A sensitive electronic search strategy using MEDLINE, EMBASE and CINAHL databases was combined with hand searching and citation tracking to identify eligible studies. Criteria for inclusion were: persons with low back pain with or without related leg symptoms, history or physical examination findings suitable for use in primary care, comparison with acceptable reference standards, and statistical reporting permitting calculation of diagnostic value. Quality assessments were made independently by two reviewers using the Quality Assessment of Diagnostic Accuracy Studies tool. Clinical examination findings that were investigated by at least two studies were included and results that met our predefined threshold of positive likelihood ratio ≥ 2 or negative likelihood ratio ≤ 0.5 were considered for the CDR.
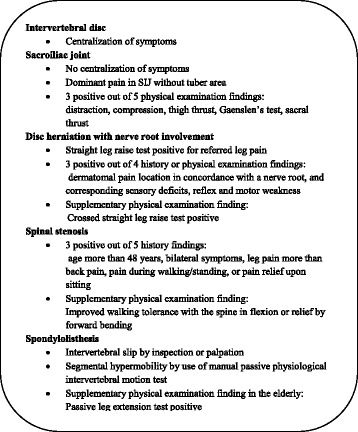
Results: Sixty-four studies satisfied our eligible criteria. We were able to construct promising CDRs for symptomatic intervertebral disc, sacroiliac joint, spondylolisthesis, disc herniation with nerve root involvement, and spinal stenosis. Single clinical test appear not to be as useful as clusters of tests that are more closely in line with clinical decision making.
Conclusions: This is the first comprehensive systematic review of diagnostic accuracy studies that evaluate clinical examination findings for their ability to identify the most common patho-anatomical disorders in the lumbar spine. In some diagnostic categories we have sufficient evidence to recommend a CDR. In others, we have only preliminary evidence that needs testing in future studies. Most findings were tested in secondary or tertiary care. Thus, the accuracy of the findings in a primary care setting has yet to be confirmed.
Keywords: Clinical decision making; Clinical examination; Diagnostic accuracy; Low back pain classification; Sensitivity and specificity.
Figures
Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Physical examination for lumbar radiculopathy due to disc herniation in patients with low-back pain.Cochrane Database Syst Rev. 2010 Feb 17;(2):CD007431. doi: 10.1002/14651858.CD007431.pub2. Cochrane Database Syst Rev. 2010. PMID: 20166095
-
Systematic review of lumbar discography as a diagnostic test for chronic low back pain.Pain Physician. 2009 May-Jun;12(3):541-59. Pain Physician. 2009. PMID: 19461822
-
A best-evidence review of diagnostic procedures for neck and low-back pain.Best Pract Res Clin Rheumatol. 2008 Jun;22(3):471-82. doi: 10.1016/j.berh.2007.12.003. Best Pract Res Clin Rheumatol. 2008. PMID: 18519100
-
Antibody tests for identification of current and past infection with SARS-CoV-2.Cochrane Database Syst Rev. 2022 Nov 17;11(11):CD013652. doi: 10.1002/14651858.CD013652.pub2. Cochrane Database Syst Rev. 2022. PMID: 36394900 Free PMC article.
Cited by
-
The Added Value of Face-to-Face Supervision to a Therapeutic Exercise-Based App in the Management of Patients with Chronic Low Back Pain: A Randomized Clinical Trial.Sensors (Basel). 2024 Jan 16;24(2):567. doi: 10.3390/s24020567. Sensors (Basel). 2024. PMID: 38257659 Free PMC article. Clinical Trial.
-
The Added Value of Radiographs in Diagnosing Knee Osteoarthritis Is Similar for General Practitioners and Secondary Care Physicians; Data from the CHECK Early Osteoarthritis Cohort.J Clin Med. 2020 Oct 21;9(10):3374. doi: 10.3390/jcm9103374. J Clin Med. 2020. PMID: 33096821 Free PMC article.
-
Nonorganic (Behavioral) Signs and Their Association With Epidural Corticosteroid Injection Treatment Outcomes and Psychiatric Comorbidity in Cervical Radiculopathy: A Multicenter Study.Mayo Clin Proc. 2023 Jun;98(6):868-882. doi: 10.1016/j.mayocp.2022.11.022. Epub 2023 Feb 15. Mayo Clin Proc. 2023. PMID: 36803892 Free PMC article.
-
Development of a Clinical Decision Aid for Chiropractic Management of Common Conditions Causing Low Back Pain in Veterans: Results of a Consensus Process.J Manipulative Physiol Ther. 2019 Nov;42(9):677-693. doi: 10.1016/j.jmpt.2019.03.009. Epub 2019 Dec 19. J Manipulative Physiol Ther. 2019. PMID: 31864769 Free PMC article.
-
Effects of spinal manipulation or mobilization as an adjunct to neurodynamic mobilization for lumbar disc herniation with radiculopathy: a randomized clinical trial.J Man Manip Ther. 2023 Dec;31(6):408-420. doi: 10.1080/10669817.2023.2192975. Epub 2023 Mar 22. J Man Manip Ther. 2023. PMID: 36950742 Free PMC article. Clinical Trial.
References
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
