

Mortality risks associated with emergency admissions during weekends and public holidays: an analysis of electronic health records
- PMID: 28499548
- PMCID: PMC5494289
- DOI: 10.1016/S0140-6736(17)30782-1
Mortality risks associated with emergency admissions during weekends and public holidays: an analysis of electronic health records
Abstract
Background: Weekend hospital admission is associated with increased mortality, but the contributions of varying illness severity and admission time to this weekend effect remain unexplored.
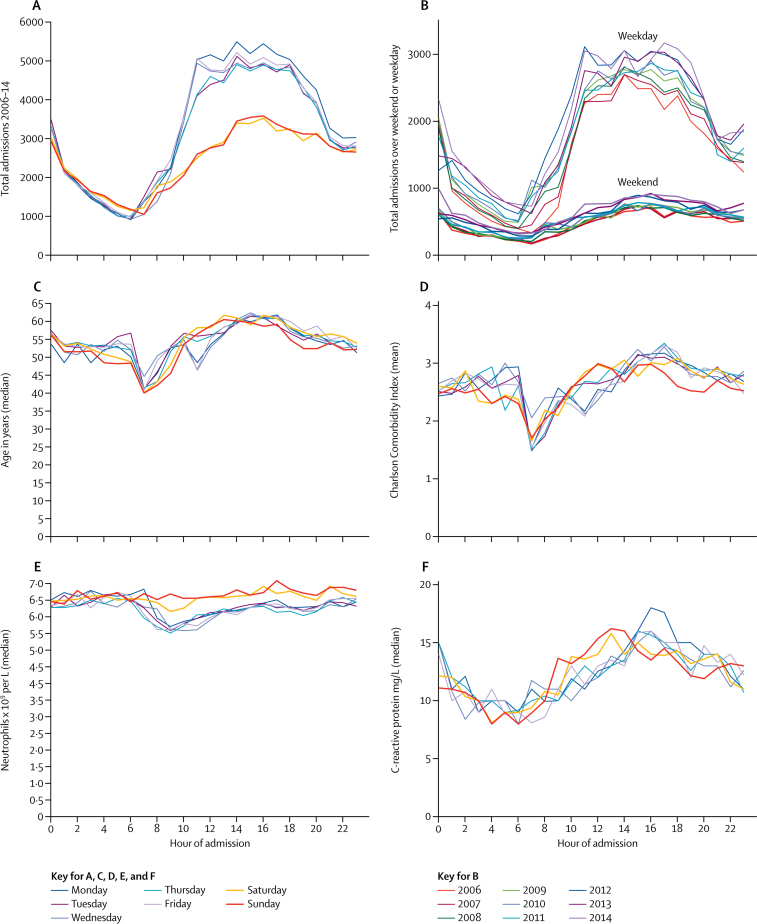
Methods: We analysed unselected emergency admissions to four Oxford University National Health Service hospitals in the UK from Jan 1, 2006, to Dec 31, 2014. The primary outcome was death within 30 days of admission (in or out of hospital), analysed using Cox models measuring time from admission. The primary exposure was day of the week of admission. We adjusted for multiple confounders including demographics, comorbidities, and admission characteristics, incorporating non-linearity and interactions. Models then considered the effect of adjusting for 15 common haematology and biochemistry test results or proxies for hospital workload.
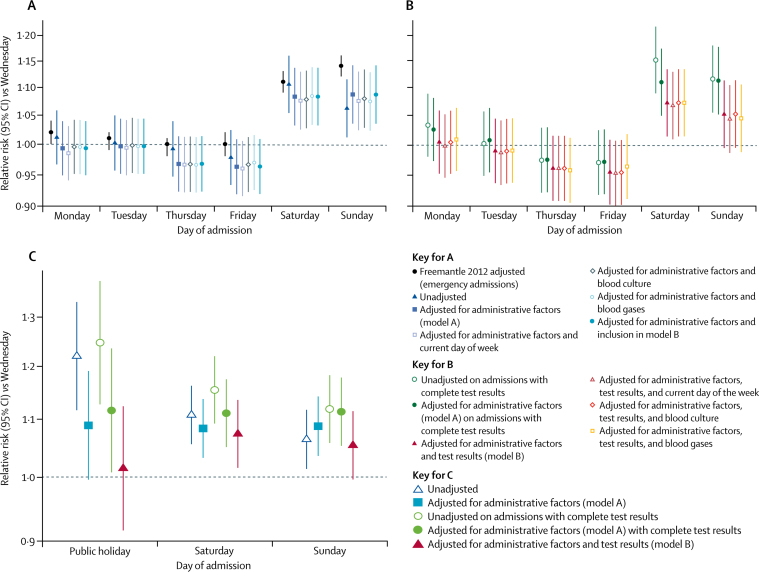
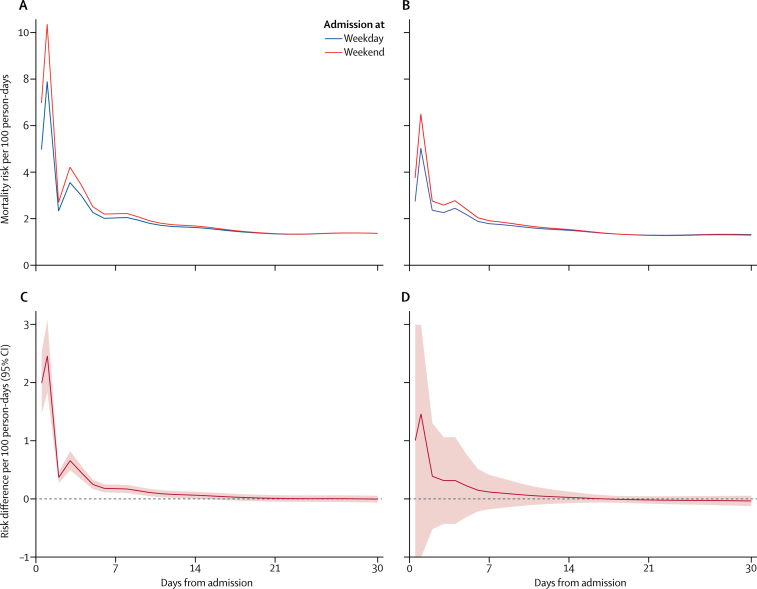
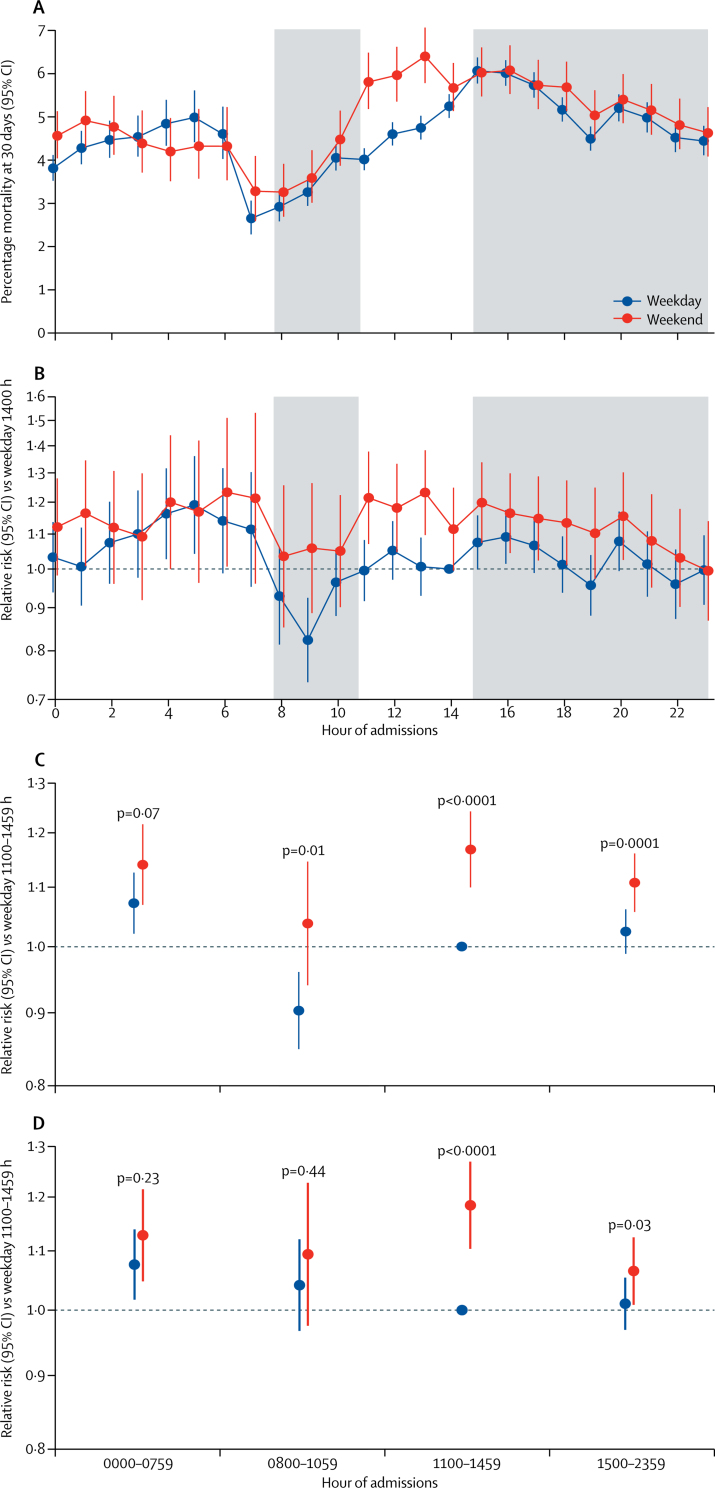
Findings: 257 596 individuals underwent 503 938 emergency admissions. 18 313 (4·7%) patients admitted as weekday energency admissions and 6070 (5·1%) patients admitted as weekend emergency admissions died within 30 days (p<0·0001). 9347 individuals underwent 9707 emergency admissions on public holidays. 559 (5·8%) died within 30 days (p<0·0001 vs weekday). 15 routine haematology and biochemistry test results were highly prognostic for mortality. In 271 465 (53·9%) admissions with complete data, adjustment for test results explained 33% (95% CI 21 to 70) of the excess mortality associated with emergency admission on Saturdays compared with Wednesdays, 52% (lower 95% CI 34) on Sundays, and 87% (lower 95% CI 45) on public holidays after adjustment for standard patient characteristics. Excess mortality was predominantly restricted to admissions between 1100 h and 1500 h (pinteraction=0·04). No hospital workload measure was independently associated with mortality (all p values >0·06).
Interpretation: Adjustment for routine test results substantially reduced excess mortality associated with emergency admission at weekends and public holidays. Adjustment for patient-level factors not available in our study might further reduce the residual excess mortality, particularly as this clustered around midday at weekends. Hospital workload was not associated with mortality. Together, these findings suggest that the weekend effect arises from patient-level differences at admission rather than reduced hospital staffing or services.
Funding: NIHR Oxford Biomedical Research Centre.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Data linkage studies can help to explain the weekend effect.Lancet. 2017 Jul 1;390(10089):8-9. doi: 10.1016/S0140-6736(17)31195-9. Epub 2017 May 9. Lancet. 2017. PMID: 28499550 No abstract available.
-
Severity of illness and the weekend effect.Lancet. 2017 Oct 14;390(10104):1734-1735. doi: 10.1016/S0140-6736(17)32642-9. Epub 2017 Oct 12. Lancet. 2017. PMID: 29047439 No abstract available.
-
Severity of illness and the weekend effect - Authors' reply.Lancet. 2017 Oct 14;390(10104):1735. doi: 10.1016/S0140-6736(17)32425-X. Epub 2017 Oct 12. Lancet. 2017. PMID: 29047441 No abstract available.
-
Acute diseases, emergency admissions and mortality during weekends: should we be worried?J Thorac Dis. 2017 Sep;9(9):2723-2727. doi: 10.21037/jtd.2017.07.87. J Thorac Dis. 2017. PMID: 29221224 Free PMC article. No abstract available.
-
Excess mortality associated with weekend hospital admissions may be due to patient-level differences, rather than reduced staffing or services.Evid Based Nurs. 2018 Apr;21(2):49. doi: 10.1136/eb-2017-102779. Epub 2018 Mar 6. Evid Based Nurs. 2018. PMID: 29510981 No abstract available.
-
The enigma of the weekend effect.J Thorac Dis. 2018 Jan;10(1):102-105. doi: 10.21037/jtd.2017.12.115. J Thorac Dis. 2018. PMID: 29600032 Free PMC article. No abstract available.
References
-
- Aylin P, Yunus A, Bottle A, Majeed A, Bell D. Weekend mortality for emergency admissions: a large, multicentre study. Qual Saf Health Care. 2010;19:213–217. - PubMed
-
- Ricciardi R, Roberts PL, Read TE, Baxter NN, Marcello PW, Schoetz DJ. Mortality rate after nonelective hospital admission. Arch Surg. 2011;146:545–551. - PubMed
-
- Barba R, Losa JE, Velasco M, Guijarro C, García de Casasola G, Zapatero A. Mortality among adult patients admitted to the hospital on weekends. Eur J Int Med. 2006;17:322–324. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
