

Lack of Efficacy of Symptoms and Medical History in Distinguishing the Degree of Eosinophilia in Nasal Polyps
- PMID: 28499777
- PMCID: PMC5784826
- DOI: 10.1016/j.jaip.2017.04.009
Lack of Efficacy of Symptoms and Medical History in Distinguishing the Degree of Eosinophilia in Nasal Polyps
Abstract
Background: Distinguishing eosinophilic nasal polyps (NP) from noneosinophilic NP will impact prognosis and therapeutic responsiveness.
Objective: To investigate the ability of clinical history and biomarkers to distinguish these conditions.
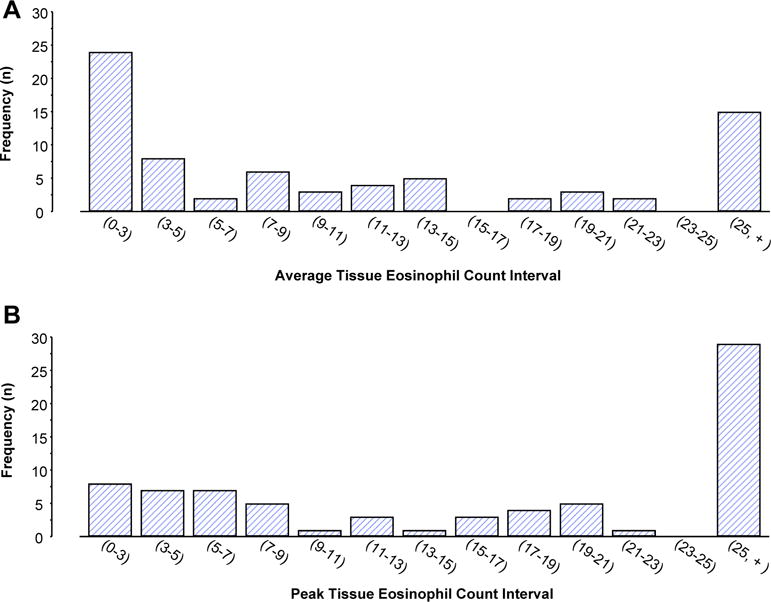
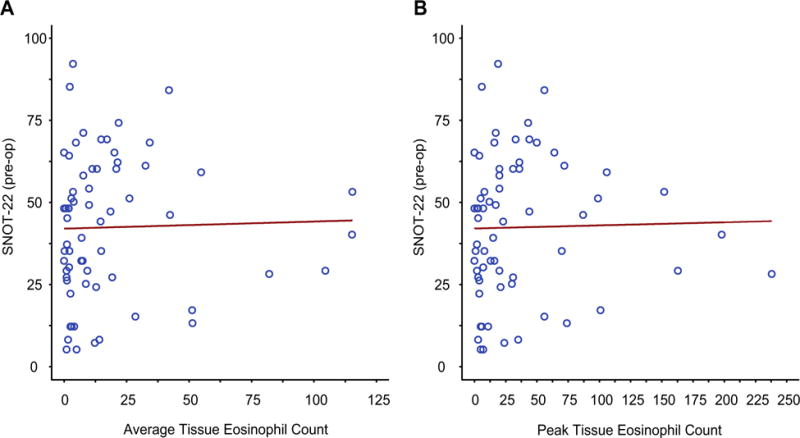
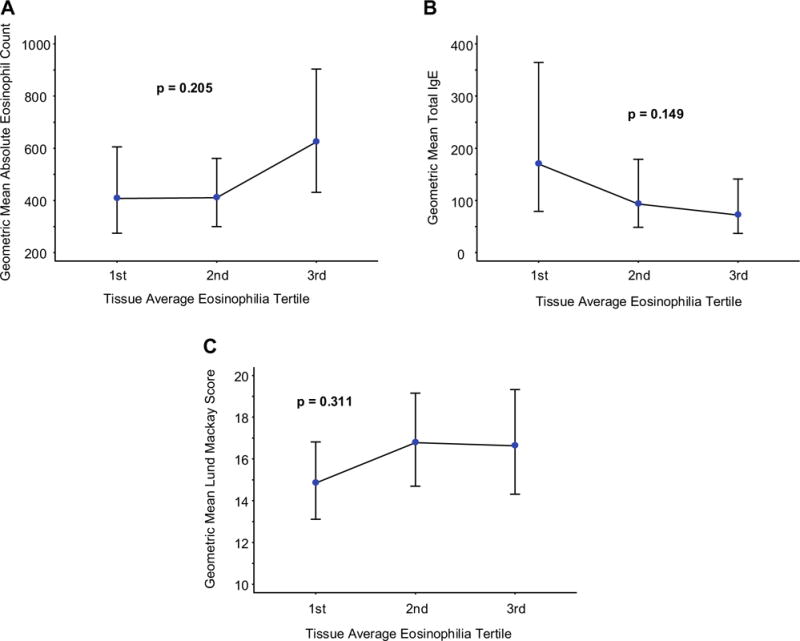
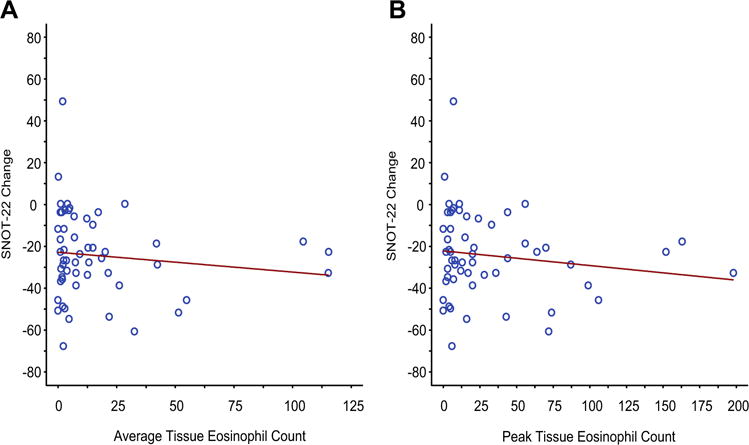
Methods: A total of 74 consecutive patients undergoing surgery for NP were enrolled. Clinical presentations were evaluated using the 22-item sinonasal outcome test (SNOT-22). Biomarkers included absolute eosinophil count, IgE, and extent of tissue hyperplasia on sinus computed tomography scan. Tissue eosinophilia was quantified in 10 random hpf and data analyzed addressing both peak and average results.
Results: No component of the SNOT-22 was predictive of tissue eosinophilia. Similarly, a medical history of allergic rhinitis, asthma, or aspirin-exacerbated respiratory disease was not predictive. An absolute eosinophil count of more than 300 was associated with NP tissue eosinophilia. In contrast, neither IgE nor extent of sinus computed tomography hyperplasia was predictive.
Conclusions: The ability to individualize therapies for NP is dependent on identifying clinical features or biomarkers of eosinophilia. However, with the exception of circulating eosinophilia, we could not identify a clinical feature or biomarker that robustly predicted the presence of tissue eosinophilia. Even more problematic, even the seeming "criterion standard" determination of tissue pathology was of limited value, as our cohort displayed a continuous spectrum of tissue eosinophil expression, making arbitrary any definitive cutoff distinguishing these conditions.
Keywords: CT scan; Chronic rhinosinusitis; Eosinophils; Nasal polyps; Sinonasal outcome test.
Copyright © 2017 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest: J. W. Steinke has received research support from the National Institutes of Health; has received lecture fees from the American Academy of Allergy, Asthma & Immunology; and receives royalties for the LUVA cell line. S. Payne has received consultancy fees from Acclarent, Medtronic, and Cook; has provided expert testimony for various legal firms; has received research support from Allakos and Knopp Bioscience; and receives royalties from Jaypee Publishing. L. Borish has received research support from the National Institutes of Health and is on the American Board of Allergy and Immunology. The rest of the authors declare that they have no relevant conflicts of interest.
Figures
Comment in
-
Nasal Polyps and Biomarkers.J Allergy Clin Immunol Pract. 2017 Nov-Dec;5(6):1589-1590. doi: 10.1016/j.jaip.2017.05.007. J Allergy Clin Immunol Pract. 2017. PMID: 29122157 No abstract available.
References
-
- Brown HM. Treatment of chronic asthma with prednisolone: significance of eosinophils in the sputum. Lancet. 1958;2:1245–7. - PubMed
-
- Cowan DC, Cowan JO, Palmay R, Williamson A, Taylor DR. Effects of steroid therapy on inflammatory cell subtypes in asthma. Thorax. 2010;65:384–90. - PubMed
-
- Ortega HG, Liu MC, Pavord ID, Brusselle GG, FitzGerald JM, Chetta A, et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med. 2014;371:1198–207. - PubMed
-
- Castro M, Zangrilli J, Wechsler ME, Bateman ED, Brusselle GG, Bardin P, et al. Reslizumab for inadequately controlled asthma with elevated blood eosinophil counts: results from two multicentre, parallel, double-blind, randomised, placebo-controlled, phase 3 trials. Lancet Respir Med. 2015;3:355–66. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
