

Glucose Peaks and the Risk of Dementia and 20-Year Cognitive Decline
- PMID: 28500217
- PMCID: PMC5481977
- DOI: 10.2337/dc16-2203
Glucose Peaks and the Risk of Dementia and 20-Year Cognitive Decline
Abstract
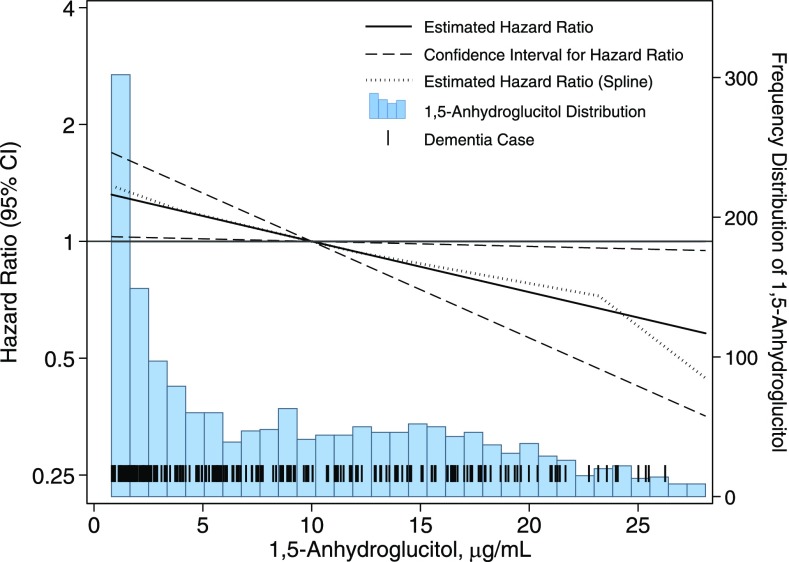
Objective: Hemoglobin A1c (HbA1c), a measure of average blood glucose level, is associated with the risk of dementia and cognitive impairment. However, the role of glycemic variability or glucose excursions in this association is unclear. We examined the association of glucose peaks in midlife, as determined by the measurement of 1,5-anhydroglucitol (1,5-AG) level, with the risk of dementia and 20-year cognitive decline.
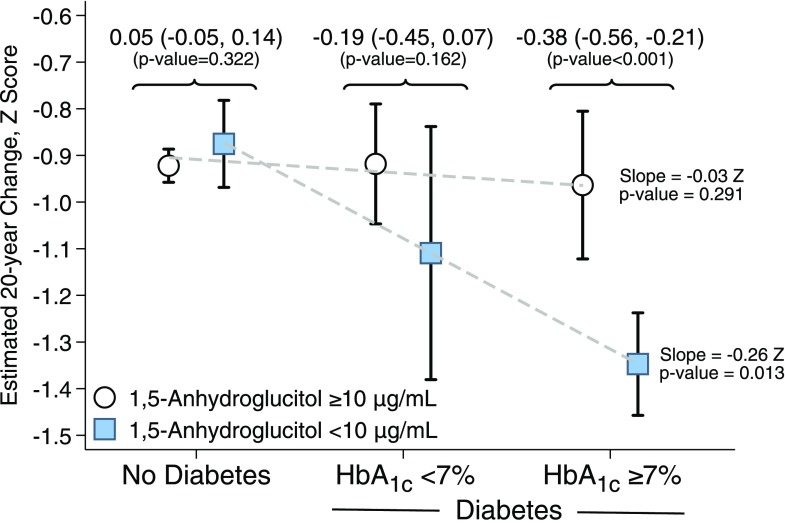
Research design and methods: Nearly 13,000 participants from the Atherosclerosis Risk in Communities (ARIC) study were examined. Dementia was ascertained from surveillance, neuropsychological testing, telephone calls with participants or their proxies, or death certificate dementia codes. Cognitive function was assessed using three neuropsychological tests at three visits over 20 years and was summarized as z scores. We used Cox and linear mixed-effects models. 1,5-AG level was dichotomized at 10 μg/mL and examined within clinical categories of HbA1c.
Results: Over a median time of 21 years, dementia developed in 1,105 participants. Among persons with diabetes, each 5 μg/mL decrease in 1,5-AG increased the estimated risk of dementia by 16% (hazard ratio 1.16, P = 0.032). For cognitive decline among participants with diabetes and HbA1c <7% (53 mmol/mol), those with glucose peaks had a 0.19 greater z score decline over 20 years (P = 0.162) compared with those without peaks. Among participants with diabetes and HbA1c ≥7% (53 mmol/mol), those with glucose peaks had a 0.38 greater z score decline compared with persons without glucose peaks (P < 0.001). We found no significant associations in persons without diabetes.
Conclusions: Among participants with diabetes, glucose peaks are a risk factor for cognitive decline and dementia. Targeting glucose peaks, in addition to average glycemia, may be an important avenue for prevention.
© 2017 by the American Diabetes Association.
Figures
References
-
- Reijmer YD, van den Berg E, Ruis C, Kappelle LJ, Biessels GJ. Cognitive dysfunction in patients with type 2 diabetes. Diabetes Metab Res Rev 2010;26:507–519 - PubMed
-
- American Diabetes Association Standards of medical care in diabetes–2016. Diabetes Care 2016;39:S1–S108
MeSH terms
Substances
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- U01 HL096812/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- P50 AG005146/AG/NIA NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- U01 HL096917/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- R01 DK089174/DK/NIDDK NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- U01 HL075572/HL/NHLBI NIH HHS/United States
- U01 HL096902/HL/NHLBI NIH HHS/United States
- T32 HL007024/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- K24 DK106414/DK/NIDDK NIH HHS/United States
- U01 HL096814/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- R01 HL070825/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- U01 HL096899/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
