

Causal Associations of Adiposity and Body Fat Distribution With Coronary Heart Disease, Stroke Subtypes, and Type 2 Diabetes Mellitus: A Mendelian Randomization Analysis
- PMID: 28500271
- PMCID: PMC5515354
- DOI: 10.1161/CIRCULATIONAHA.116.026560
Causal Associations of Adiposity and Body Fat Distribution With Coronary Heart Disease, Stroke Subtypes, and Type 2 Diabetes Mellitus: A Mendelian Randomization Analysis
Abstract
Background: The implications of different adiposity measures on cardiovascular disease etiology remain unclear. In this article, we quantify and contrast causal associations of central adiposity (waist-to-hip ratio adjusted for body mass index [WHRadjBMI]) and general adiposity (body mass index [BMI]) with cardiometabolic disease.
Methods: Ninety-seven independent single-nucleotide polymorphisms for BMI and 49 single-nucleotide polymorphisms for WHRadjBMI were used to conduct Mendelian randomization analyses in 14 prospective studies supplemented with coronary heart disease (CHD) data from CARDIoGRAMplusC4D (Coronary Artery Disease Genome-wide Replication and Meta-analysis [CARDIoGRAM] plus The Coronary Artery Disease [C4D] Genetics; combined total 66 842 cases), stroke from METASTROKE (12 389 ischemic stroke cases), type 2 diabetes mellitus from DIAGRAM (Diabetes Genetics Replication and Meta-analysis; 34 840 cases), and lipids from GLGC (Global Lipids Genetic Consortium; 213 500 participants) consortia. Primary outcomes were CHD, type 2 diabetes mellitus, and major stroke subtypes; secondary analyses included 18 cardiometabolic traits.
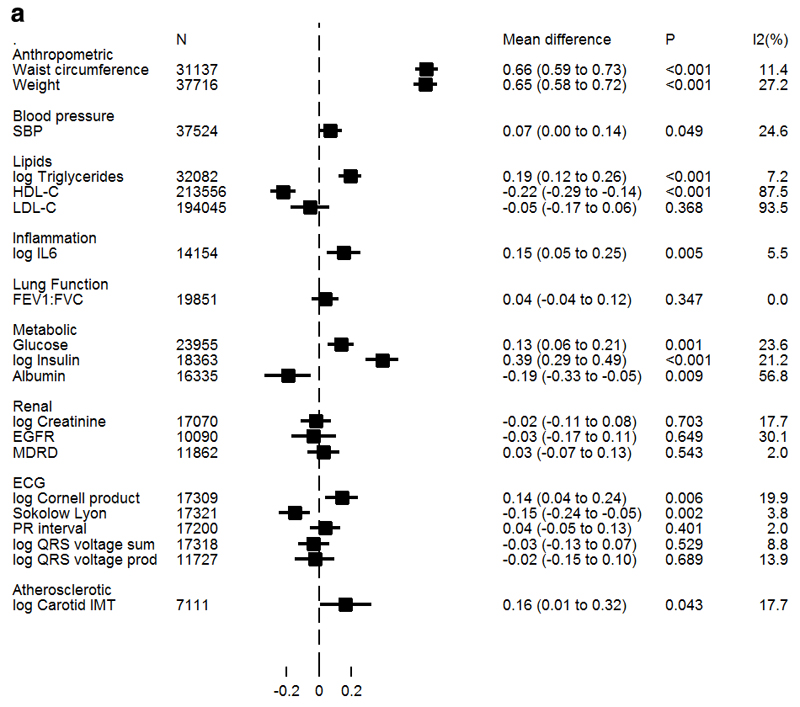
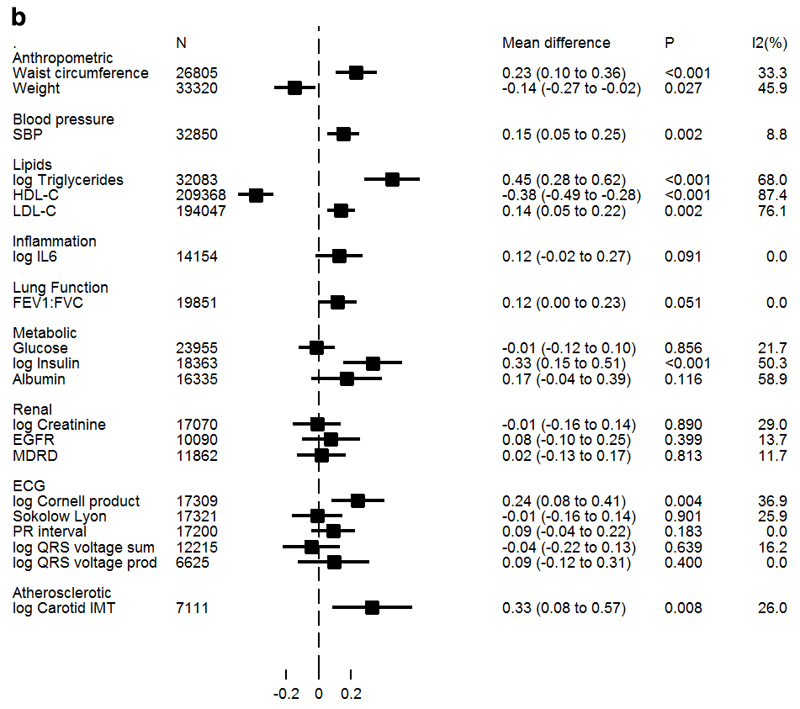
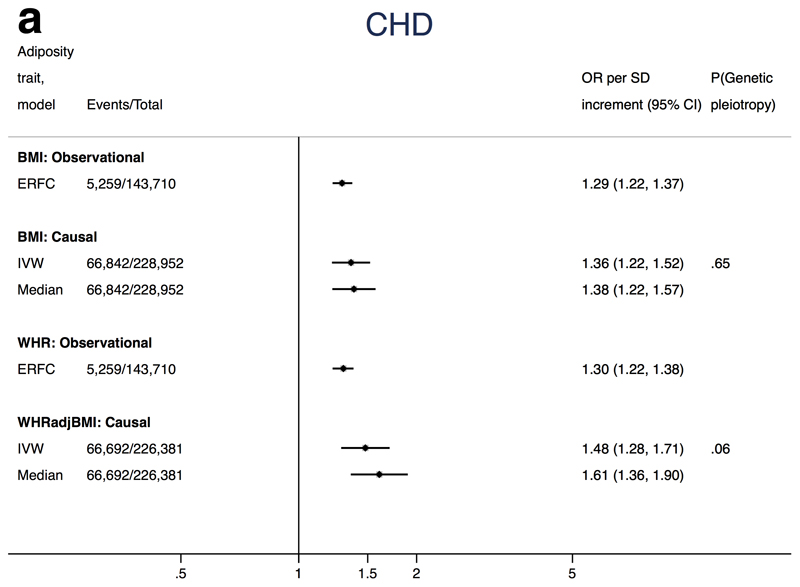
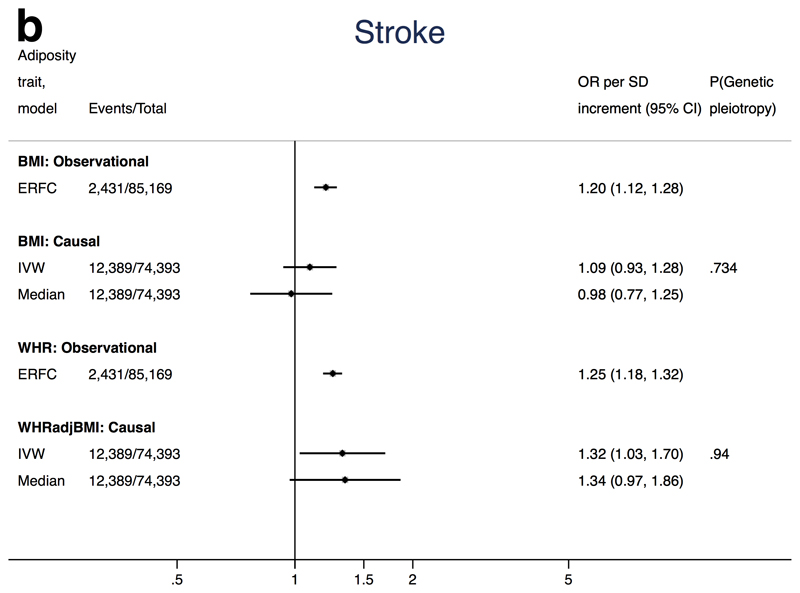
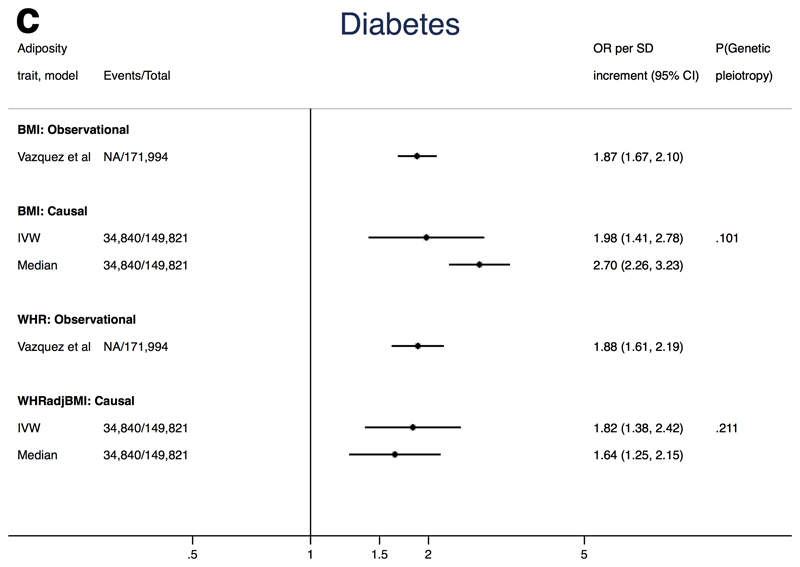
Results: Each one standard deviation (SD) higher WHRadjBMI (1 SD≈0.08 U) associated with a 48% excess risk of CHD (odds ratio [OR] for CHD, 1.48; 95% confidence interval [CI], 1.28-1.71), similar to findings for BMI (1 SD≈4.6 kg/m2; OR for CHD, 1.36; 95% CI, 1.22-1.52). Only WHRadjBMI increased risk of ischemic stroke (OR, 1.32; 95% CI, 1.03-1.70). For type 2 diabetes mellitus, both measures had large effects: OR, 1.82 (95% CI, 1.38-2.42) and OR, 1.98 (95% CI, 1.41-2.78) per 1 SD higher WHRadjBMI and BMI, respectively. Both WHRadjBMI and BMI were associated with higher left ventricular hypertrophy, glycemic traits, interleukin 6, and circulating lipids. WHRadjBMI was also associated with higher carotid intima-media thickness (39%; 95% CI, 9%-77% per 1 SD).
Conclusions: Both general and central adiposity have causal effects on CHD and type 2 diabetes mellitus. Central adiposity may have a stronger effect on stroke risk. Future estimates of the burden of adiposity on health should include measures of central and general adiposity.
Keywords: Mendelian randomization analysis; adiposity; body fat distribution; body mass index; coronary artery disease; stroke; waist-hip ratio.
© 2017 American Heart Association, Inc.
Figures
References
-
- Wormser D, Kaptoge S, Di Angelantonio E, Wood AM, Pennells L, Thompson A, Sarwar N, Kizer JR, Lawlor DA, Nordestgaard BG, Ridker P, et al. Separate and combined associations of body-mass index and abdominal adiposity with cardiovascular disease: collaborative analysis of 58 prospective studies. Lancet. 2011;377:1085–1095. doi: 10.1016/S0140-6736(11)60105-0. - DOI - PMC - PubMed
-
- Vazquez G, Duval S, Jacobs DR, Jr, Silventoinen K. Comparison of body mass index, waist circumference, and waist/hip ratio in predicting incident diabetes: a meta-analysis. Epidemiol Rev. 2007;29:115–128. - PubMed
-
- Yusuf S, Hawken S, Ounpuu S, Bautista L, Franzosi MG, Commerford P, Lang CC, Rumboldt Z, Onen CL, Lisheng L, Tanomsup S, et al. Obesity and the risk of myocardial infarction in 27,000 participants from 52 countries: a case-control study. Lancet. 2005;366:1640–1649. - PubMed
-
- Canoy D, Cairns BJ, Balkwill A, Wright FL, Green J, Reeves G, Beral V, Million Women Study C Coronary heart disease incidence in women by waist circumference within categories of body mass index. Eur J Prev Cardiol. 2013;20:759–762. - PubMed
-
- O'Donnell MJ, Chin SL, Rangarajan S, Xavier D, Liu L, Zhang H, Rao-Melacini P, Zhang X, Pais P, Agapay S, Lopez-Jaramillo P, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. 2016;388:761–775. - PubMed
MeSH terms
Grants and funding
- G9521010/MRC_/Medical Research Council/United Kingdom
- G1001799/MRC_/Medical Research Council/United Kingdom
- RG/08/008/25291/BHF_/British Heart Foundation/United Kingdom
- PG/13/66/30442/BHF_/British Heart Foundation/United Kingdom
- G0802432/MRC_/Medical Research Council/United Kingdom
- MC_UU_12019/1/MRC_/Medical Research Council/United Kingdom
- MR/N01104X/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_12013/1/MRC_/Medical Research Council/United Kingdom
- MR/K006584/1/MRC_/Medical Research Council/United Kingdom
- G0600237/MRC_/Medical Research Council/United Kingdom
- MC_UU_12013/5/MRC_/Medical Research Council/United Kingdom
- MC_UU_12013/8/MRC_/Medical Research Council/United Kingdom
- G0801228/MRC_/Medical Research Council/United Kingdom
- MR/N01104X/2/MRC_/Medical Research Council/United Kingdom
- RG/10/12/28456/BHF_/British Heart Foundation/United Kingdom
- SP/13/6/30554/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
