

Tips and tricks for a safe and effective image-guided percutaneous renal tumour ablation
- PMID: 28500486
- PMCID: PMC5438321
- DOI: 10.1007/s13244-017-0555-4
Tips and tricks for a safe and effective image-guided percutaneous renal tumour ablation
Abstract
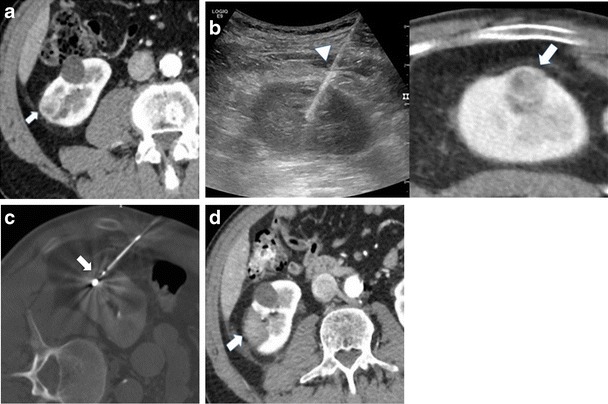
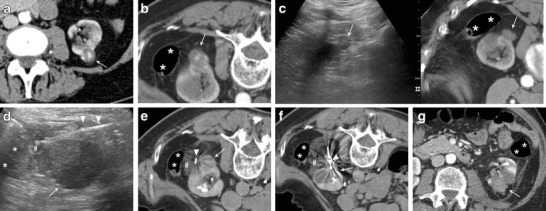
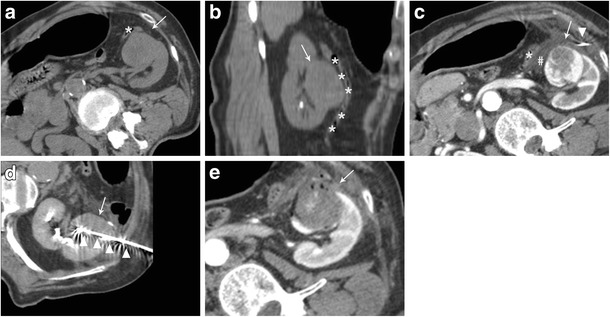
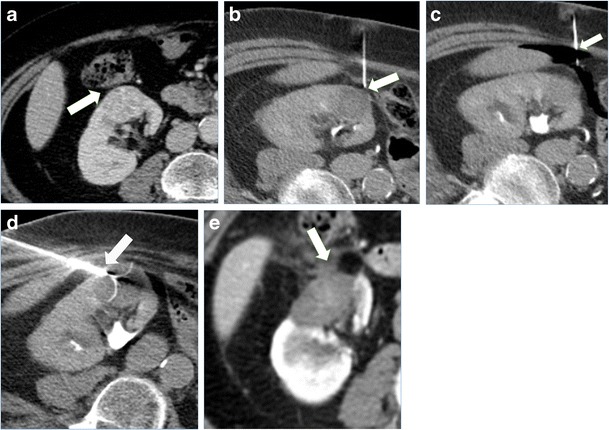
Image-guide thermal ablations are nowadays increasingly used to provide a minimally invasive treatment to patients with renal tumours, with reported good clinical results and low complications rate. Different ablative techniques can be applied, each with some advantages and disadvantages according to the clinical situation. Moreover, percutaneous ablation of renal tumours might be complex in cases where there is limited access for image guidance or a close proximity to critical structures, which can be unintentionally injured during treatment. In the present paper we offer an overview of the most commonly used ablative techniques and of the most important manoeuvres that can be applied to enhance the safety and effectiveness of percutaneous image-guided renal ablation. Emphasis is given to the different technical aspects of cryoablation, radiofrequency ablation, and microwave ablation, on the ideal operating room setting, optimal image guidance, application of fusion imaging and virtual navigation, and contrast enhanced ultrasound in the guidance and monitoring of the procedure. Moreover, a series of protective manoeuvre that can be used to avoid damage to surrounding sensitive structures is presented. A selection of cases of image-guided thermal ablation of renal tumours in which the discussed technique were used is presented and illustrated.
Teaching points: • Cryoablation, radiofrequency and microwave ablation have different advantages and disadvantages. • US, CT, fusion imaging, and CEUS increase an effective image-guidance. • Different patient positioning and external compression may increase procedure feasibility. • Hydrodissection and gas insufflation are useful to displace surrounding critical structures. • Cold pyeloperfusion can reduce the thermal damage to the collecting system.
Keywords: Image guidance; Image-guided tumour ablation; Protective manoeuvres; Renal ablation; Renal tumours.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
