

Epidemiological analysis and follow-up of human rhinovirus infection in children with asthma exacerbation
- PMID: 28500687
- PMCID: PMC7167043
- DOI: 10.1002/jmv.24850
Epidemiological analysis and follow-up of human rhinovirus infection in children with asthma exacerbation
Abstract
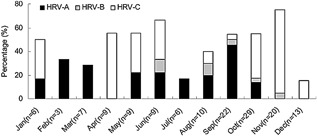
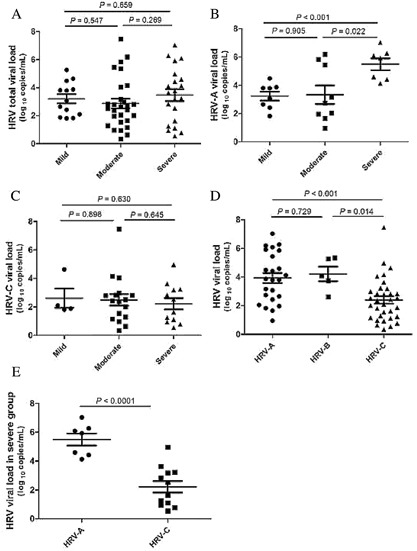
To determine the prevalence of human rhinovirus (HRV) infection in children with acute asthma exacerbations, investigation of HRV viral load and severity of asthma exacerbations is also required. Nasopharyngeal aspirates and swabs were collected and assessed for respiratory viruses. HRV-positive samples were sequenced to identify types and determine viral load. Outpatients with asthma exacerbations underwent follow-up evaluations, their swabs were collected and clinical outcomes were recorded at their next clinic visit 4 weeks later. One hundred forty-three inpatients and 131 outpatients, including 88 patients with asthma exacerbations and 43 controls with stable asthma were recruited. HRV-A was mainly detected in September and February (45.5% and 33.3%, respectively), while HRV-C was mainly detected in November and April (70.0% and 55.6%, respectively). HRV-C was the primary type and was primarily found in inpatients with severe asthma exacerbations. HRV-A viral load in the group of inpatients with severe exacerbations was higher than in the mild and moderate groups (P < 0.001 and P = 0.022). The HRV-A viral load of both inpatients and outpatients was higher than that of HRV-C (P < 0.001 and P = 0.036). The main genotypes were HRV-C53 and HRV-A20 among inpatients, and this genotype caused more severe clinical manifestations. HRV persisted for no more than 4 weeks, and their symptoms or signs of disease were well-controlled well. HRV-C was most frequently detected in asthma exacerbations. HRV-A with high viral load led to severe asthma exacerbations.
Keywords: asthma exacerbations; children; human rhinoviruses; type; viral load.
© 2017 Wiley Periodicals, Inc.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures


References
-
- Busse WW, Lemanske RF. Asthma. N Engl J Med. 2001; 344:350–362. - PubMed
-
- Garbino J, Gerbase MW, Wunderli W, et al. Lower respiratory viral illnesses: improved diagnosis by molecular methods and clinical impact. Am J Respir Crit Care Med. 2004; 170:1197–1203. - PubMed
-
- Glezen WP, Greenberg SB, Atmar RL, Piedra PA, Couch RB. Impact of respiratory virus infections on persons with chronic underlying conditions. JAMA. 2000; 283:499–505. - PubMed
-
- Johnston SL. Innate immunity in the pathogenesis of virus induced asthma exacerbations. Proc Am Thorac Soc. 2007; 4:267–270. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
