

Exercise and other non-pharmaceutical interventions for cancer-related fatigue in patients during or after cancer treatment: a systematic review incorporating an indirect-comparisons meta-analysis
- PMID: 28501804
- PMCID: PMC5931245
- DOI: 10.1136/bjsports-2016-096422
Exercise and other non-pharmaceutical interventions for cancer-related fatigue in patients during or after cancer treatment: a systematic review incorporating an indirect-comparisons meta-analysis
Abstract
Aim: To assess the relative effects of different types of exercise and other non-pharmaceutical interventions on cancer-related fatigue (CRF) in patients during and after cancer treatment.
Design: Systematic review and indirect-comparisons meta-analysis.
Data sources: Articles were searched in PubMed, Cochrane CENTRAL and published meta-analyses.
Eligibility criteria for selecting studies: Randomised studies published up to January 2017 evaluating different types of exercise or other non-pharmaceutical interventions to reduce CRF in any cancer type during or after treatment.
Study appraisal and synthesis: Risk of bias assessment with PEDro criteria and random effects Bayesian network meta-analysis.
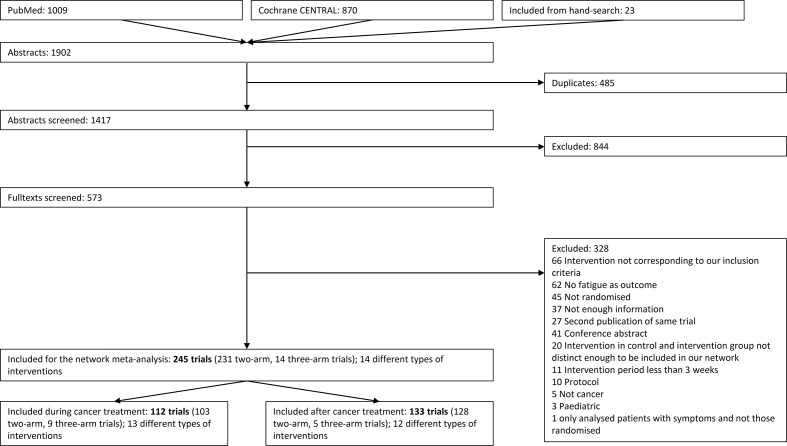
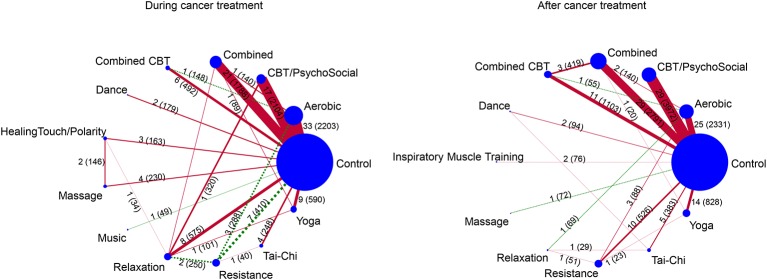
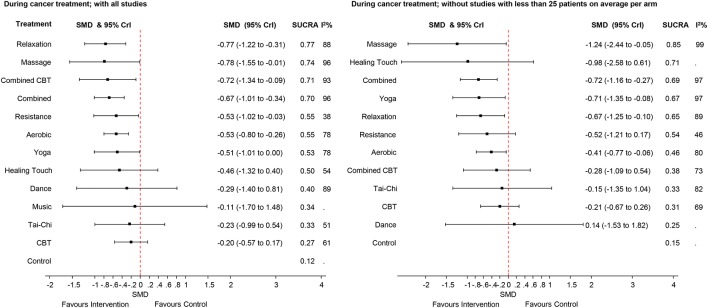
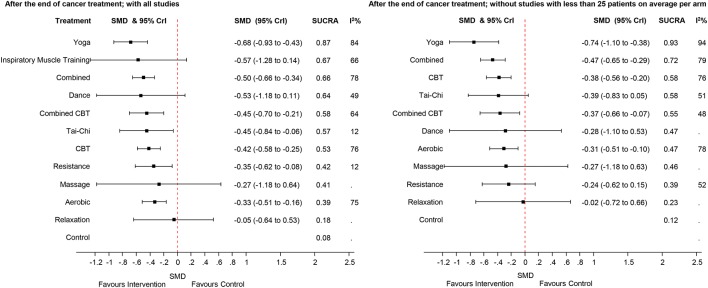
Results: We included 245 studies. Comparing the treatments with usual care during cancer treatment, relaxation exercise was the highest ranked intervention with a standardisedmean difference (SMD) of -0.77 (95% Credible Interval (CrI) -1.22 to -0.31), while massage (-0.78; -1.55 to -0.01), cognitive-behavioural therapy combined with physical activity (combined CBT, -0.72; -1.34 to -0.09), combined aerobic and resistance training (-0.67; -1.01 to -0.34), resistance training (-0.53; -1.02 to -0.03), aerobic (-0.53; -0.80 to -0.26) and yoga (-0.51; -1.01 to 0.00) all had moderate-to-large SMDs. After cancer treatment, yoga showed the highest effect (-0.68; -0.93 to -0.43). Combined aerobic and resistance training (-0.50; -0.66 to -0.34), combined CBT (-0.45; -0.70 to -0.21), Tai-Chi (-0.45; -0.84 to -0.06), CBT (-0.42; -0.58 to -0.25), resistance training (-0.35; -0.62 to -0.08) and aerobic (-0.33; -0.51 to -0.16) showed all small-to-moderate SMDs.
Conclusions: Patients can choose among different effective types of exercise and non-pharmaceutical interventions to reduce CRF.
Keywords: cancer related fatigue; exercise; indirect comparison meta-analysis.; network meta-analysis; non-pharmaceutical interventions.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- NCCN NCCN. Cancer-Related Fatigue : Network N, NCCN clinical practice guidelines in oncology (NCCN guidelines). Version 1. 2016 ed: NCCN National Comprehensive Cancer Network, 2016:1–56.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical