

Superior Canal Dehiscence Syndrome: Lessons from the First 20 Years
- PMID: 28503164
- PMCID: PMC5408023
- DOI: 10.3389/fneur.2017.00177
Superior Canal Dehiscence Syndrome: Lessons from the First 20 Years
Abstract
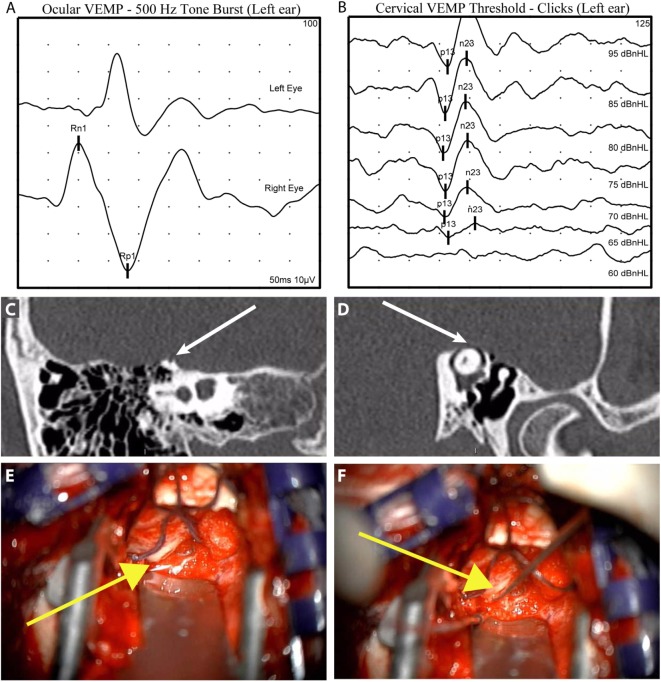
Superior semicircular canal dehiscence syndrome was first reported by Lloyd Minor and colleagues in 1998. Patients with a dehiscence in the bone overlying the superior semicircular canal experience symptoms of pressure or sound-induced vertigo, bone conduction hyperacusis, and pulsatile tinnitus. The initial series of patients were diagnosed based on common symptoms, a physical examination finding of eye movements in the plane of the superior semicircular canal when ear canal pressure or loud tones were applied to the ear, and high-resolution computed tomography imaging demonstrating a dehiscence in the bone over the superior semicircular canal. Research productivity directed at understanding better methods for diagnosing and treating this condition has substantially increased over the last two decades. We now have a sound understanding of the pathophysiology of third mobile window syndromes, higher resolution imaging protocols, and several sensitive and specific diagnostic tests. Furthermore, we have a treatment (surgical occlusion of the superior semicircular canal) that has demonstrated efficacy. This review will highlight some of the fundamental insights gained in SCDS, propose diagnostic criteria, and discuss future research directions.
Keywords: autophony; labyrinth diseases; superior semicircular canal dehiscence syndrome; vertigo; vestibular diseases.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources