

Hierarchical Models for Multiple, Rare Outcomes Using Massive Observational Healthcare Databases
- PMID: 28503249
- PMCID: PMC5423675
- DOI: 10.1002/sam.11324
Hierarchical Models for Multiple, Rare Outcomes Using Massive Observational Healthcare Databases
Abstract
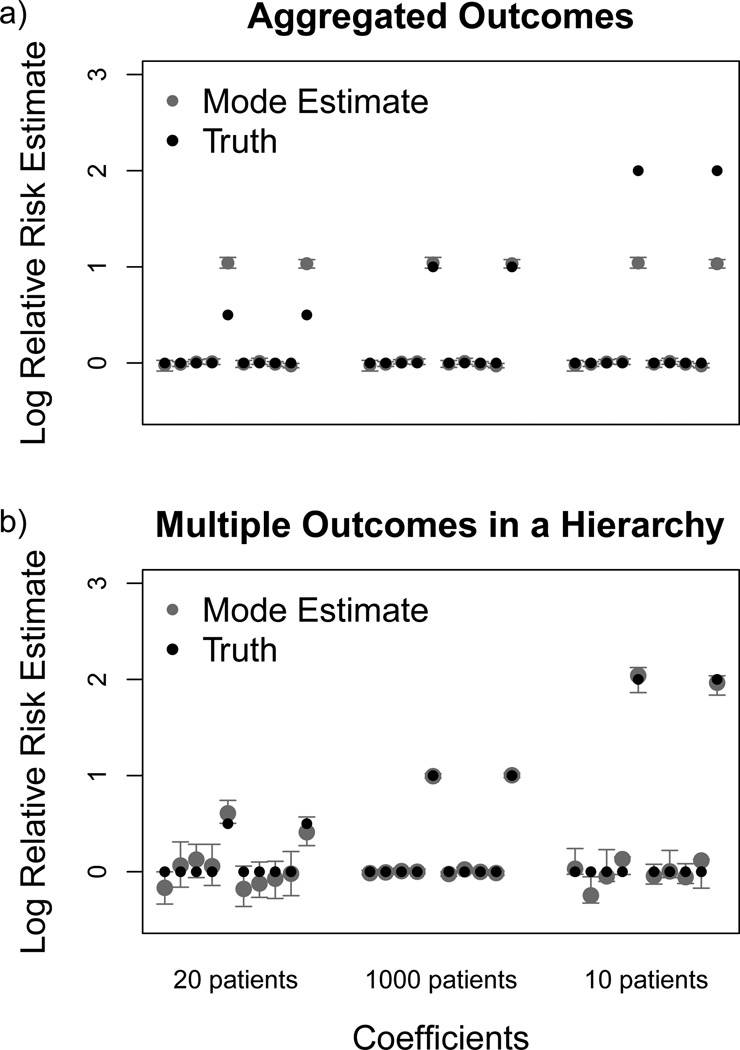
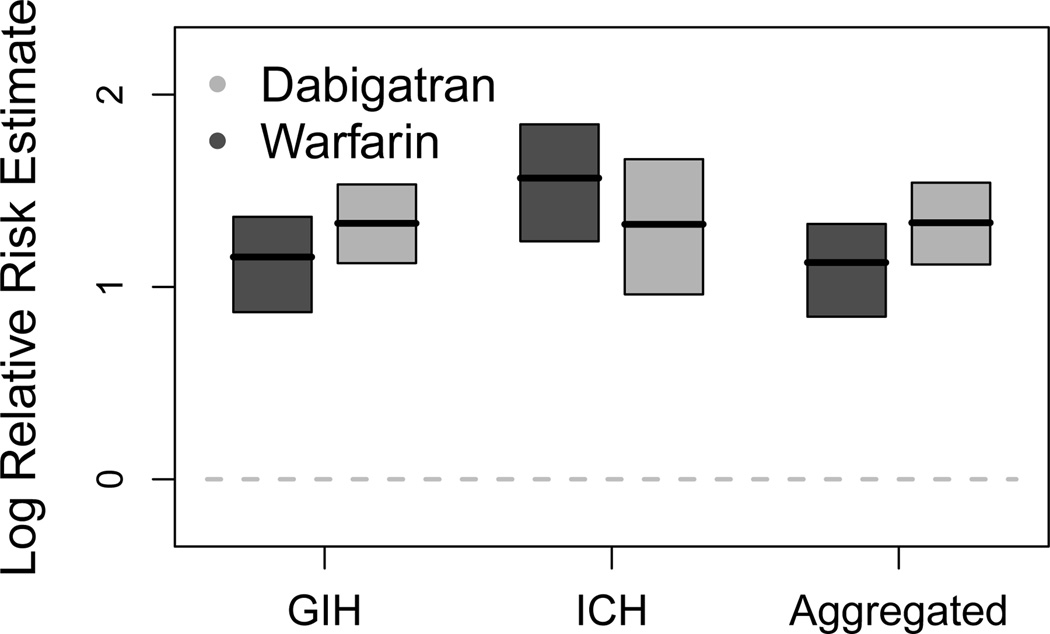
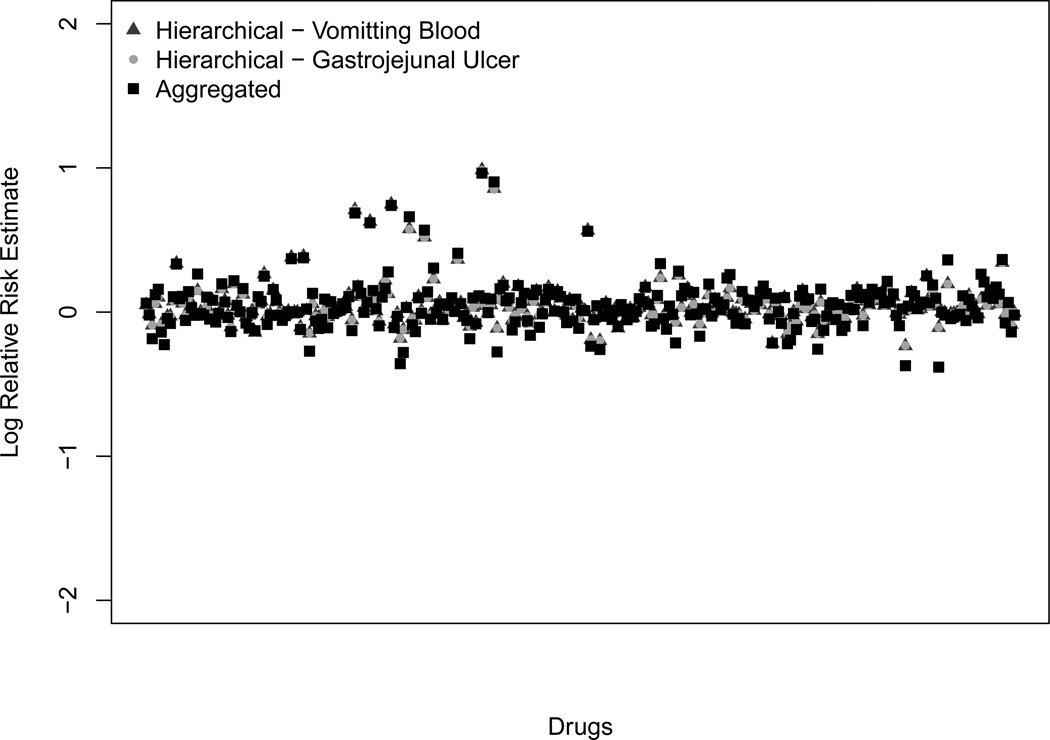
Clinical trials often lack power to identify rare adverse drug events (ADEs) and therefore cannot address the threat rare ADEs pose, motivating the need for new ADE detection techniques. Emerging national patient claims and electronic health record databases have inspired post-approval early detection methods like the Bayesian self-controlled case series (BSCCS) regression model. Existing BSCCS models do not account for multiple outcomes, where pathology may be shared across different ADEs. We integrate a pathology hierarchy into the BSCCS model by developing a novel informative hierarchical prior linking outcome-specific effects. Considering shared pathology drastically increases the dimensionality of the already massive models in this field. We develop an efficient method for coping with the dimensionality expansion by reducing the hierarchical model to a form amenable to existing tools. Through a synthetic study we demonstrate decreased bias in risk estimates for drugs when using conditions with different true risk and unequal prevalence. We also examine observational data from the MarketScan Lab Results dataset, exposing the bias that results from aggregating outcomes, as previously employed to estimate risk trends of warfarin and dabigatran for intracranial hemorrhage and gastrointestinal bleeding. We further investigate the limits of our approach by using extremely rare conditions. This research demonstrates that analyzing multiple outcomes simultaneously is feasible at scale and beneficial.
Figures
References
-
- Cannon CP, Cannon PJ. COX-2 inhibitors and cardiovascular risk. Science. 2012;336(6087):1386–1387. - PubMed
-
- Charlton B, Redberg R. The trouble with dabigatran. BMJ. 2014;349:g4681. - PubMed
-
- Connolly SJ, Ezekowitz MD, Yusuf Salim, Eikelboom J, Oldgren J, Parekh A, Pogue J, Reilly PA, Themeles E, Varrone J, Wang S, Alings M, Xavier D, Zhu J, Diaz R, Lewis BS, Darius H, Diener HC, Joyner CD, Wallentin L the RE-LY Steering Committee and Investigators. Dabigatran versus warfarin in patients with atrial fibrillation. NEJM. 2009;361(12):228–235. - PubMed
-
- Connolly SJ, Ezekowitz MD, Yusuf S, Reilly PA, Wallentin L. Newly identified events in the re-ly trial. NEJM. 2010;363:1875–1876. - PubMed
-
- Crooks CJ, Prieto-Merino D, Evans SJW. Identifying adverse events of vaccines using a Bayesian method of medically guided information sharing. Drug Safety. 2012;35(1):61–78. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous