

Cell-free DNA copy number variations in plasma from colorectal cancer patients
- PMID: 28504856
- PMCID: PMC5537711
- DOI: 10.1002/1878-0261.12077
Cell-free DNA copy number variations in plasma from colorectal cancer patients
Abstract
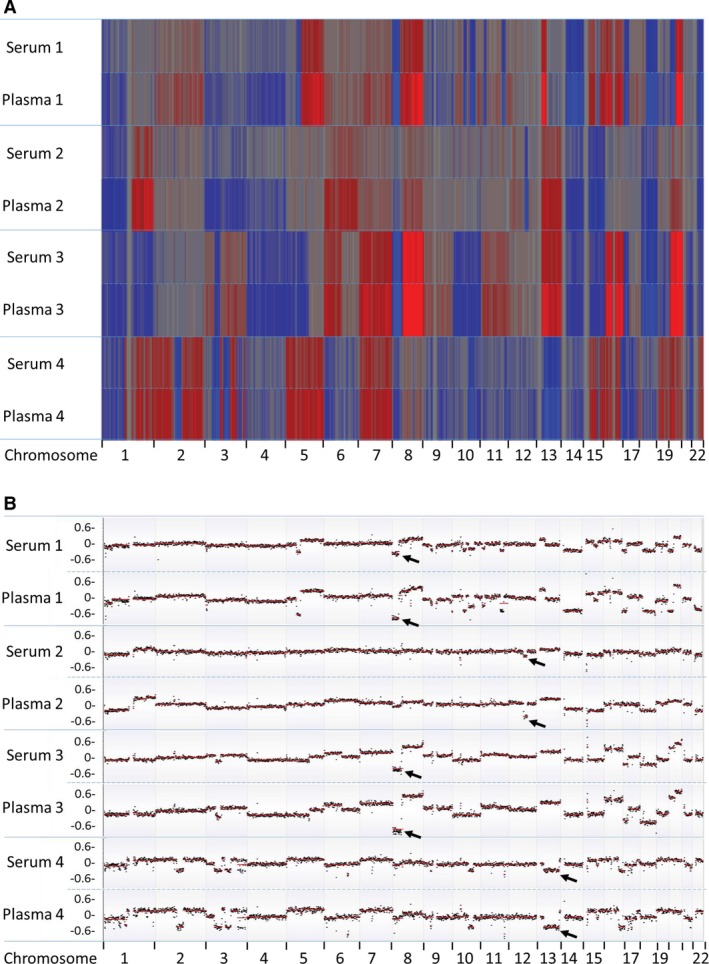
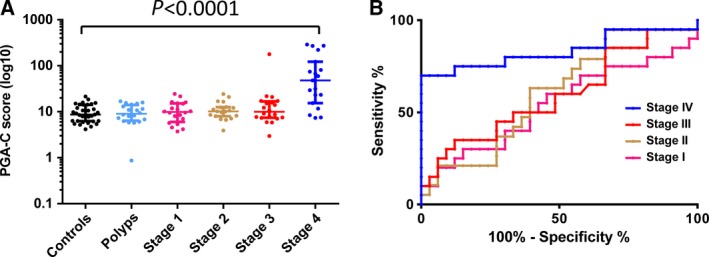
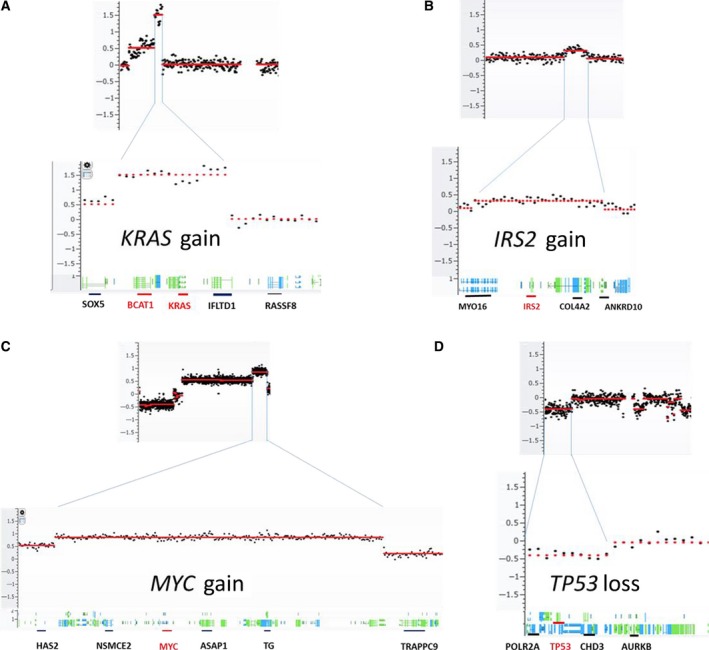
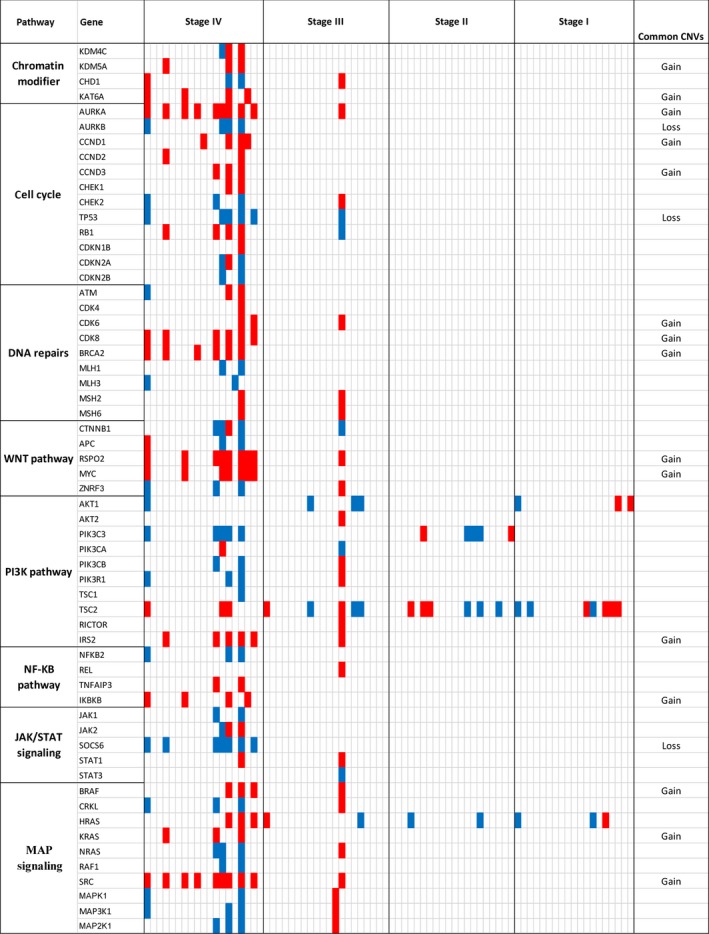
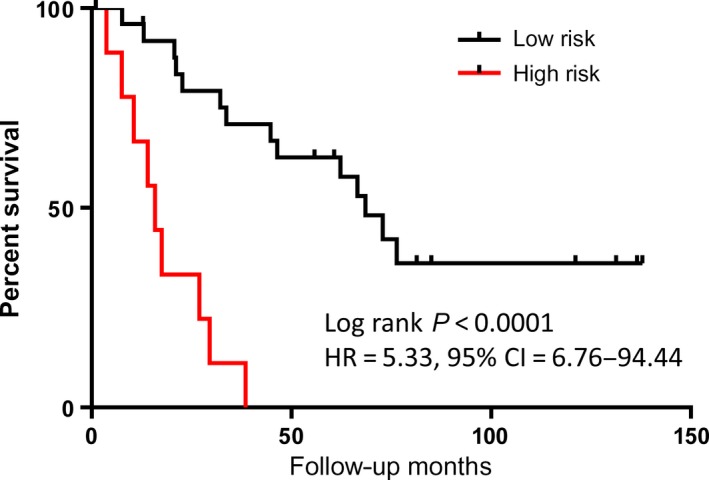
To evaluate the clinical utility of cell-free DNA (cfDNA), we performed whole-genome sequencing to systematically examine plasma cfDNA copy number variations (CNVs) in a cohort of patients with colorectal cancer (CRC, n = 80), polyps (n = 20), and healthy controls (n = 35). We initially compared cfDNA yield in 20 paired serum-plasma samples and observed significantly higher cfDNA concentration in serum (median = 81.20 ng, range 7.18-500 ng·mL-1 ) than in plasma (median = 5.09 ng, range 3.76-62.8 ng·mL-1 ) (P < 0.0001). However, tumor-derived cfDNA content was significantly lower in serum than in matched plasma samples tested. With ~10 million reads per sample, the sequencing-based copy number analysis showed common CNVs in multiple chromosomal regions, including amplifications on 1q, 8q, and 5q and deletions on 1p, 4q, 8p, 17p, 18q, and 22q. Copy number changes were also evident in genes critical to the cell cycle, DNA repair, and WNT signaling pathways. To evaluate whether cumulative copy number changes were associated with tumor stages, we calculated plasma genomic abnormality in colon cancer (PGA-C) score by summing the most significant CNVs. The PGA-C score showed predictive performance with an area under the curve from 0.54 to 0.84 for CRC stages I-IV. Locus-specific copy number analysis identified nine genomic regions where CNVs were significantly associated with survival in stage III-IV CRC patients. A multivariate model using six of nine genomic regions demonstrated a significant association of high-risk score with shorter survival (HR = 5.33, 95% CI = 6.76-94.44, P < 0.0001). Our study demonstrates the importance of using plasma (rather than serum) to test tumor-related genomic variations. Plasma cfDNA-based tests can capture tumor-specific genetic changes and may provide a measurable classifier for assessing clinical outcomes in advanced CRC patients.
Keywords: cell-free DNA; colon cancer; copy number variation; next-generation sequencing; survival.
© 2017 The Authors. Published by FEBS Press and John Wiley & Sons Ltd.
Figures
References
-
- Bretthauer M (2011) Colorectal cancer screening. J Intern Med 270, 87–98. - PubMed
-
- Carvalho B, Postma C, Mongera S, Hopmans E, Diskin S, van de Wiel MA, van Criekinge W, Thas O, Matthai A, Cuesta MA et al (2009) Multiple putative oncogenes at the chromosome 20q amplicon contribute to colorectal adenoma to carcinoma progression. Gut 58, 79–89. - PubMed
-
- Chao M and Gibbs P (2009) Caution is required before recommending routine carcinoembryonic antigen and imaging follow‐up for patients with early‐stage colon cancer. J Clin Oncol 27, e279–e280. author reply e281. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
