

Strongyloides seroprevalence before and after an ivermectin mass drug administration in a remote Australian Aboriginal community
- PMID: 28505198
- PMCID: PMC5444847
- DOI: 10.1371/journal.pntd.0005607
Strongyloides seroprevalence before and after an ivermectin mass drug administration in a remote Australian Aboriginal community
Abstract
Background: Strongyloides seroprevalence is hyper-endemic in many Australian Aboriginal and Torres Strait Islander communities, ranging from 35-60%. We report the impact on Strongyloides seroprevalence after two oral ivermectin mass drug administrations (MDAs) delivered 12 months apart in a remote Australian Aboriginal community.
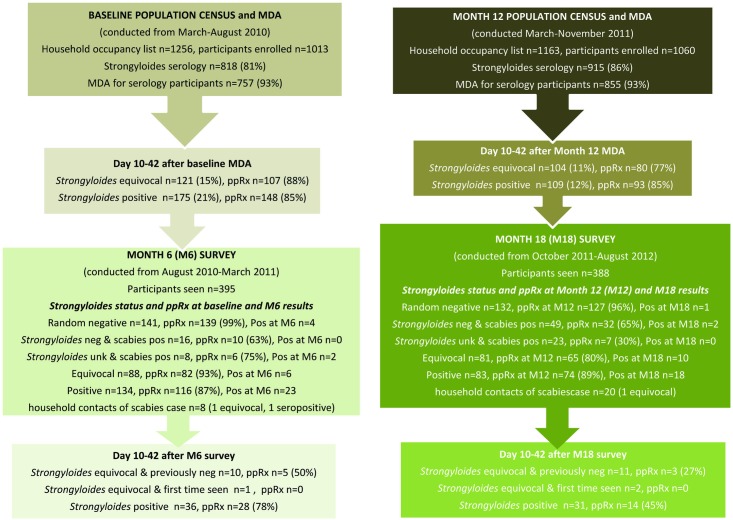
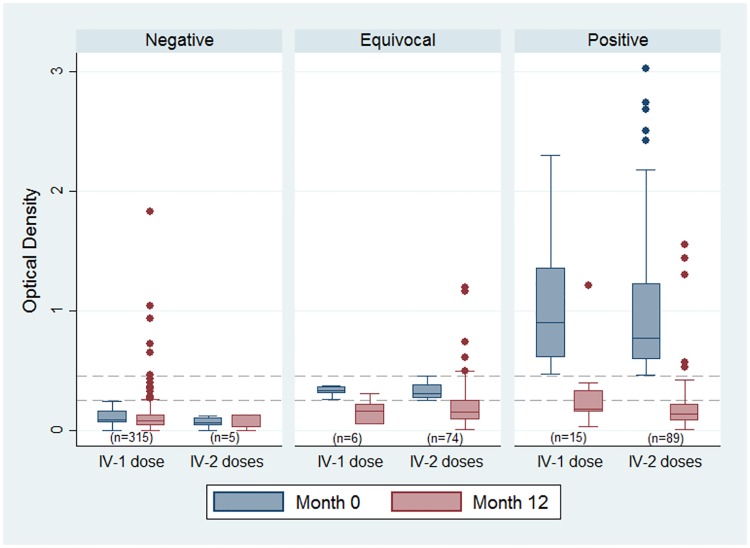
Methods: Utilizing a before and after study design, we measured Strongyloides seroprevalence through population census with sequential MDAs at baseline and month 12. Surveys at months 6 and 18 determined changes in serostatus. Serodiagnosis was undertaken by ELISA that used sonicated Strongyloides ratti antigen to detect anti-Strongyloides IgG. Non-pregnant participants weighing ≥15 kg were administered a single 200 μg/kg ivermectin dose, repeated after 10-42 days if Strongyloides and/or scabies was diagnosed; others followed a standard alternative algorithm. A questionnaire on clinical symptoms was administered to identify adverse events from treatment and self-reported symptoms associated with serostatus.
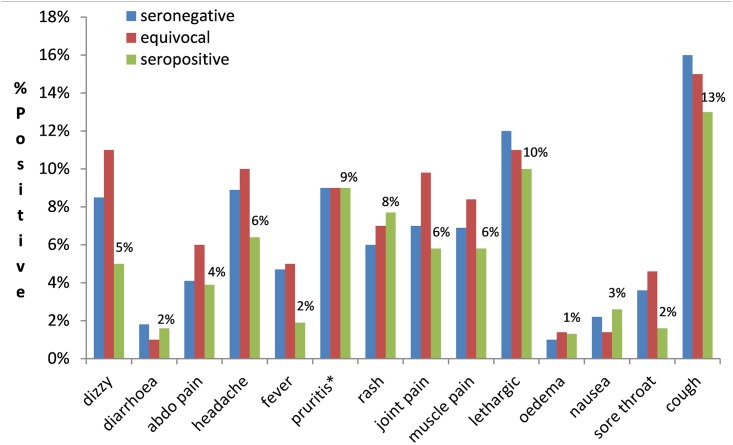
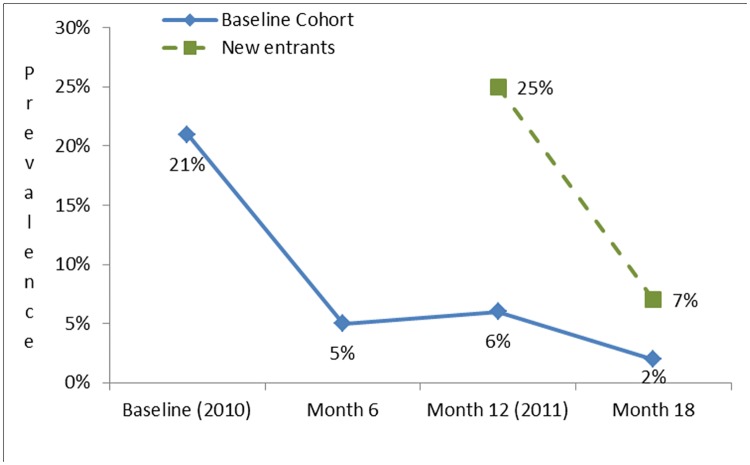
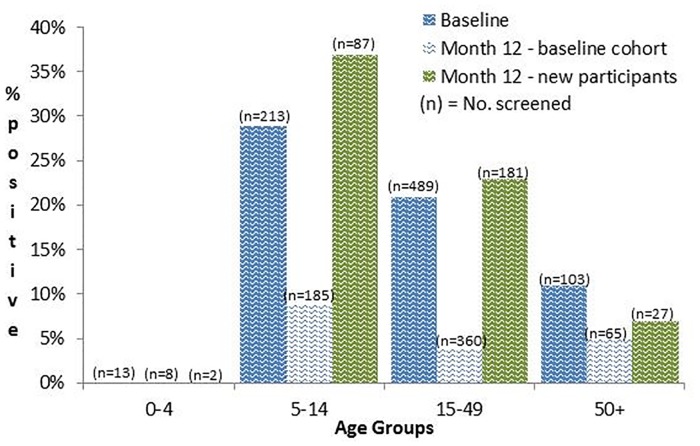
Findings: We surveyed 1013 participants at the baseline population census and 1060 (n = 700 from baseline cohort and 360 new entrants) at month 12. Strongyloides seroprevalence fell from 21% (175/818) at baseline to 5% at month 6. For participants from the baseline cohort this reduction was sustained at month 12 (34/618, 6%), falling to 2% at month 18 after the second MDA. For new entrants to the cohort at month 12, seroprevalence reduced from 25% (75/297) to 7% at month 18. Strongyloides positive seroconversions for the baseline cohort six months after each MDA were 2.5% (4/157) at month 6 and 1% at month 18, whilst failure to serorevert remained unchanged at 18%. At 12 months, eosinophilia was identified in 59% of baseline seropositive participants and 89% of seropositive new entrants, compared with 47%baseline seronegative participants and 51% seronegative new entrants. Seropositivity was not correlated with haemoglobin or any self-reported clinical symptoms. Clinical symptoms ascertained on the day of treatment and 24-72 hrs after, did not identify any adverse events.
Significance: Two community ivermectin MDAs delivered 12 months apart by trained Aboriginal researchers in collaboration with non-Indigenous researchers resulted in a sustained and significant reduction in Strongyloides seroprevalence over 18 months. Similar reductions were seen in the baseline cohort and new entrants.
Conflict of interest statement
The authors have declared that no competing interests exist. WP and EM are employed by Miwatj Aboriginal Health Corporation, an independent, Aboriginal-controlled health service administered by a Board of Directors.
Figures
References
-
- Dorris M, Viney ME, Blaxter ML (2002) Molecular phylogenetic analysis of the genus Strongyloides and related nematodes. Int J Parasitol 32: 1507–1517. - PubMed
-
- Flannery G, White N, editors (1993) Immunological parameters in northeast Arnhem Land Aborigines: consequences of changing settlement and lifestyles: Cambridge Uni. Press; 202–220 p.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
