

Advanced Human Immunodeficiency Virus Disease in Botswana Following Successful Antiretroviral Therapy Rollout: Incidence of and Temporal Trends in Cryptococcal Meningitis
- PMID: 28505328
- PMCID: PMC5850554
- DOI: 10.1093/cid/cix430
Advanced Human Immunodeficiency Virus Disease in Botswana Following Successful Antiretroviral Therapy Rollout: Incidence of and Temporal Trends in Cryptococcal Meningitis
Abstract
Background: Botswana has a well-developed antiretroviral therapy (ART) program that serves as a regional model. With wide ART availability, the burden of advanced human immunodeficiency virus (HIV) and associated opportunistic infections would be expected to decline. We performed a nationwide surveillance study to determine the national incidence of cryptococcal meningitis (CM), and describe characteristics of cases during 2000-2014 and temporal trends at 2 national referral hospitals.
Methods: Cerebrospinal fluid data from all 37 laboratories performing meningitis diagnostics in Botswana were collected from the period 2000-2014 to identify cases of CM. Basic demographic and laboratory data were recorded. Complete national data from 2013-2014 were used to calculate national incidence using UNAIDS population estimates. Temporal trends in cases were derived from national referral centers in the period 2004-2014.
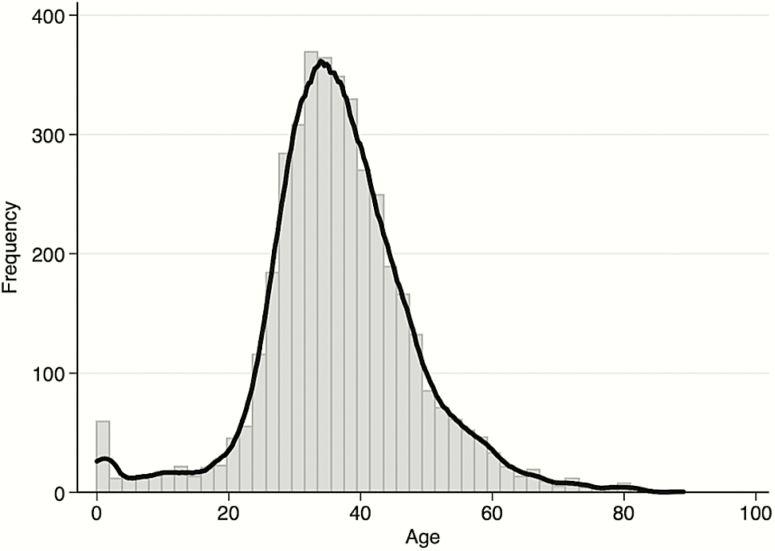
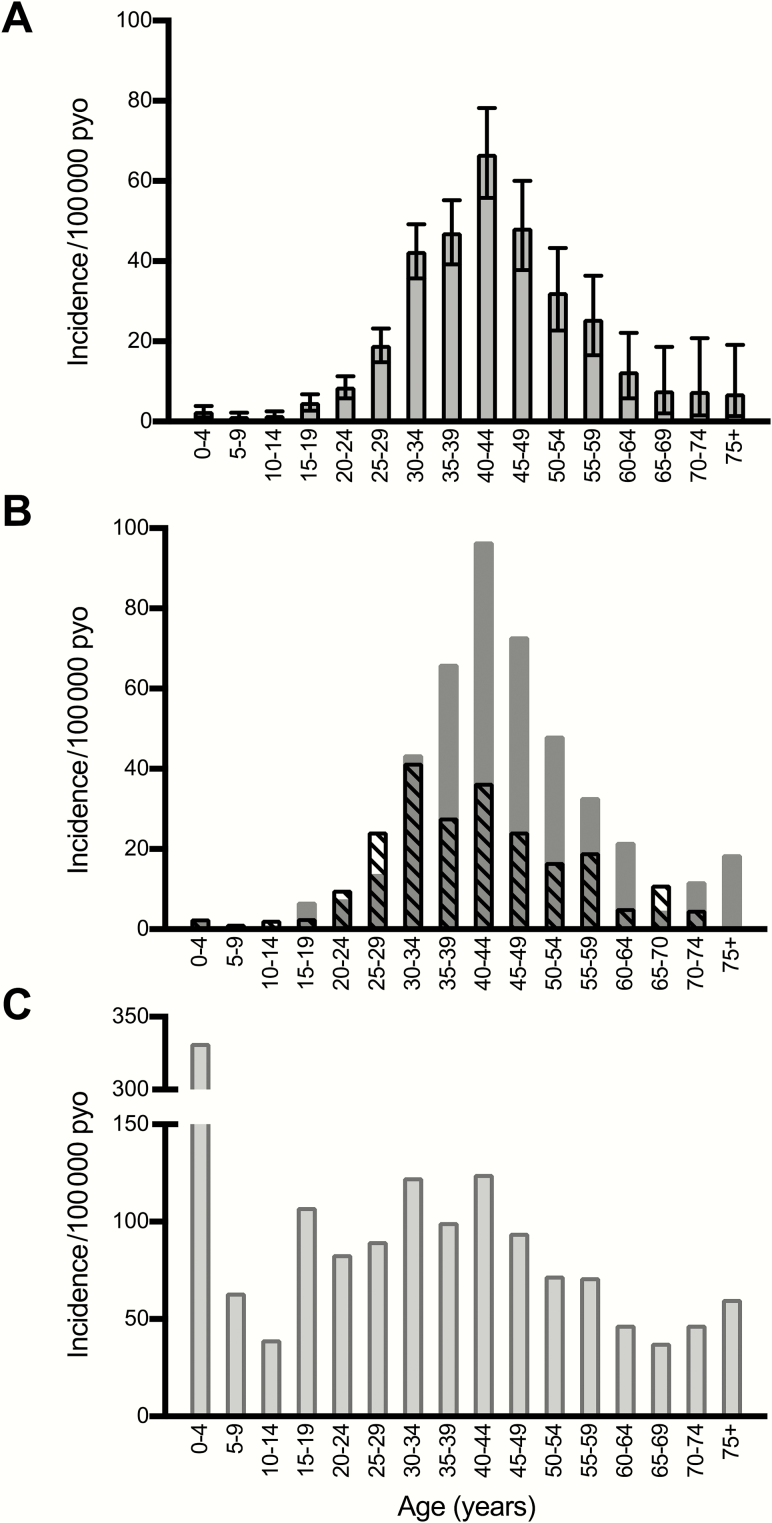
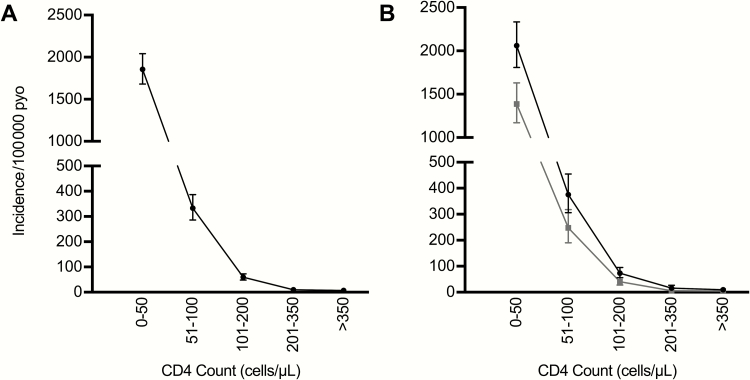
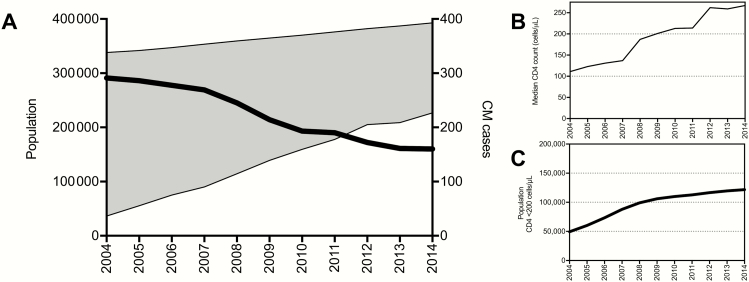
Results: A total of 5296 episodes of CM were observed in 4702 individuals; 60.6% were male, and median age was 36 years. Overall 2013-2014 incidence was 17.8 (95% confidence interval [CI], 16.6-19.2) cases per 100000 person-years. In the HIV-infected population, incidence was 96.8 (95% CI, 90.0-104.0) cases per 100000 person-years; male predominance was seen across CD4 strata. At national referral hospitals, cases decreased during 2007-2009 but stabilized during 2010-2014.
Conclusions: Despite excellent ART coverage in Botswana, there is still a substantial burden of advanced HIV, with 2013-2014 incidence of CM comparable to pre-ART era rates in South Africa. Our findings suggest that a key population of individuals, often men, is developing advanced disease and associated opportunistic infections due to a failure to effectively engage in care, highlighting the need for differentiated care models.
Keywords: Botswana; HIV; cryptococcal meningitis; incidence; sub-Saharan Africa.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Farahani M, Vable A, Lebelonyane R et al. Outcomes of the Botswana national HIV/AIDS treatment programme from 2002 to 2010: a longitudinal analysis. Lancet Glob Health 2014; 2:e44–50. - PubMed
-
- Botswana Ministry of Health. 2012 Botswana national HIV & AIDS treatment guidelines Available at: https://hivpolicywatch.org/duremaps/data/guidelines/BotswanaARTguideline.... Accessed 28 March 2017.
-
- Botswana Ministry of Health. Botswana national HIV/AIDS treatment guidelines: 2008 version Available at: http://www.moh.gov.bw/Publications/HIVAIDS treatment guidelines.pdf. Accessed 28 March 2017.
-
- Karim SA. Is the UNAIDS target sufficient for HIV control in Botswana? Lancet HIV 2016; 3:e195–6. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
